Table of contents
- Main points
- Statistician’s quote
- Things you need to know about this release
- People can expect to live over three quarters of their life in good health
- Health state life expectancies differ up to 3 years between UK countries
- Health state life expectancies at birth differ by up to 19.6 years within countries
- Life expectancy at age 65 differ by up to 5.6 years within countries
- What are health expectancies?
- How do we calculate health state life expectancies?
- How do constituent countries health expectancies compare to other estimates?
- Quality and Information
1. Main points
A newborn baby boy could expect to live 79.2 years and a newborn baby girl 82.9 years if mortality rates remain the same as they were in the UK in 2013 to 2015 throughout their lives.
Life expectancy for the UK is higher in 2013 to 2015 compared to 2009 to 2011 but the proportion of life spent in good health is falling, due to the improvement in life expectancy exceeding that of healthy life expectancy.
A newborn baby boy could expect to live 63.1 years in good health if they experienced the same health status rates as observed between 2013 and 2015, 0.8 years lower than it was for baby girls. For males, healthy life expectancy increased by 0.4 years since 2009 to 2011 but for females it remained static at 63.9 years.
Disability-free life expectancy at birth was 62.7 years for males in 2013 to 2015, 0.3 years higher than it was for females.
Females continue to have a higher number of years in good health than males, despite this males live a higher proportion of their lives in good health and disability-free.
The highest life expectancy at birth for males is 83.4 years in Kensington and Chelsea, the lowest is 73.4 years in Glasgow City. The highest estimate for females is 86.7 years in Hart (South East of England); the lowest is 78.7 in West Dunbartonshire.
For males at birth across the UK, Rutland had the highest estimates for healthy and disability-free life expectancy (71.1 and 70.8 years respectively). The lowest estimates are 54.0 years in good health in Tower Hamlets and Causeway Coast and Glens and 51.3 years disability-free in Blaenau Gwent.
For females at birth across the UK, the highest estimate of years in good health was 74.6 years for Orkney Islands and the lowest was 47.8 years in Antrim and Newtownabbey. Wokingham had the highest years spent disability-free with 71.8 and Antrim and Newtownabbey had the lowest with females on average living 52.0 years disability-free.
Back to table of contents2. Statistician’s quote
“Improvements to healthcare and living healthier lives mean that as a nation we are living longer and newborn boys and girls can expect to live for 79 and 83 years respectively. However while we are living longer we are spending a smaller proportion of our overall lives in good health which puts a greater challenge on health services.”
Sarah Caul, Senior Health Researcher
Back to table of contents3. Things you need to know about this release
This bulletin combines and extends four previous Health State Life Expectancy publications: Life Expectancy at Birth and at Age 65 by Local Areas in England and Wales, Healthy life expectancy at birth and age 65 by upper tier local authority and area deprivation: England, Disability-Free Life Expectancy by Upper Tier Local Authority: England and Health Expectancies at Birth and at Age 65 in the UK.
The estimates that are produced in this report are created for comparison to lower geographies. National Life Tables estimates produced by us will differ from the UK and constituent country estimates produced in this report and cannot be compared to the lower geography estimates as methods differ. More information can be found in the "How do constituent countries health expectancies compare to other estimates?" section.
Lower geography life expectancy estimates for Scotland and Northern Ireland have been calculated using the same method as for England and Wales. Responsibility for the production of other lower geography statistics for Scotland and Northern Ireland are with the National Records Scotland (NRS) and Northern Ireland Statistics and Research Agency (NISRA) respectively.
Other lower geography healthy and disability-free life expectancy estimates for Wales, Scotland and Northern Ireland can be found on Public Health Wales Observatory (PHW), Scottish Public Health Observatory (ScotPHO) and Department of Health Northern Ireland websites. More information can be found in the "How do constituent countries health expectancies compare to other estimates?" section.
This analysis uses a new upper age group of 90 and over which was previously set at 85 and over. The impact of this can be seen in the methods change paper published earlier this year. The methods paper also notes the change in health state life expectancies which utilises the census data. There is a slight difference in Northern Ireland methodology as the census data for lower geographies is supplied with the age group 0 to 4 instead of 0 and 1 to 4.
Life expectancy estimates for the UK, constituent countries, and all lower geographies in Great Britain have been revised using the new 90 and over upper age group from 2001 to 2003. UK, constituent countries and English region and upper tier local authorities health expectancies have been revised from the period 2009 to 2011.
Life expectancy at a given age for an area is the average number of years a person would live, if he or she experienced the particular area’s age-specific mortality rates for that time period throughout his or her life. It makes no allowance for any later actual or projected changes in mortality. In practice, death rates of the area are likely to change in the future, so period life expectancy does not therefore give the number of years someone could actually expect to live. Also, people may live in other areas for at least some part of their lives.
Back to table of contents4. People can expect to live over three quarters of their life in good health
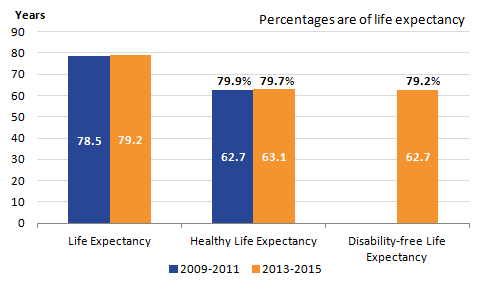
If newborn boys in the UK experienced the same mortality rates that were observed over the period 2013 to 2015 they could expect to live for 79.2 years. This is an increase from 78.5 years if newborns experienced the observed mortality rates during the period 2009 to 2011. Males are living longer lives but are living a smaller proportion in good health compared to the earlier period (79.9% compared to 79.7%). This is because healthy life expectancy is rising at a slower pace than overall life expectancy. Figures 1 and 2 show life expectancy and healthy life expectancy for 2009 to 2011 and 2013 to 2015 and disability-free life expectancy (DFLE) for 2013 to 2015 for each sex.
The disability questions on the Annual Population Survey (APS) have undergone a number of changes since 2010 and as a result estimates are not comparable over time. More details can be found in section 7.
No comparisons have been made in this bulletin of DFLE over time.
Figure 1: Health state life expectancies at birth, males, United Kingdom, 2009 to 2011 and 2013 to 2015
Source: Office for National Statistics
Download this image Figure 1: Health state life expectancies at birth, males, United Kingdom, 2009 to 2011 and 2013 to 2015
.png (9.3 kB) .xls (26.6 kB)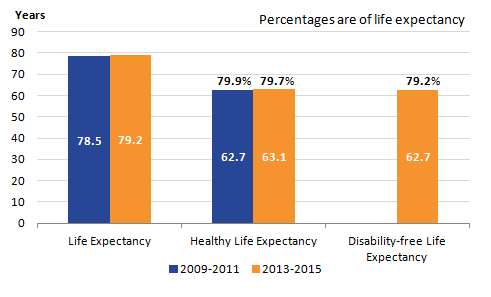{kind=link}
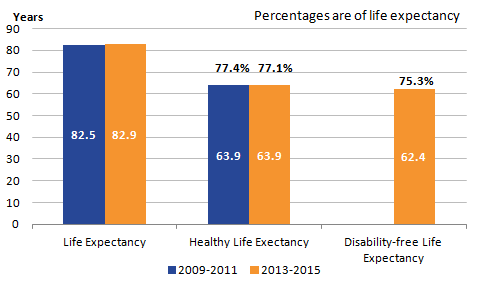
Figure 2: Health state life expectancies at birth, females, United Kingdom, 2009 to 2011 and 2013 to 2015
Source: Office for National Statistics
Download this image Figure 2: Health state life expectancies at birth, females, United Kingdom, 2009 to 2011 and 2013 to 2015
.png (7.6 kB) .xls (26.6 kB)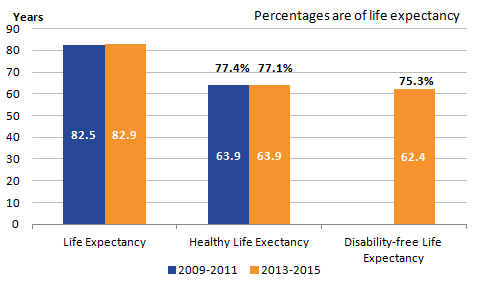{kind=link}
As shown in figure 2, life expectancy for females has also seen a small rise, 82.9 years in 2013 to 2015 compared to 82.5 years in 2009 to 2011. Female life expectancy remains higher than for males and the proportion spent in good health (77.1%) and disability-free (75.3%) remains lower among females compared to males. The proportion of life spent in good health is lower in 2013 to 2015 compared to 2009 to 2011 due to life expectancy rising and healthy life expectancy staying the same.
Males life expectancy has increased by more years (0.7 years) compared to females (0.4 years), although the changes are small, they are statistically significant differences.
Life expectancy estimates from 2001 to 2003, healthy and disability-free life expectancy from 2009 to 2011 for the UK for males and females at all ages can be found in the accompanying reference tables.
Since the UK has an ageing population, with more men and women in the oldest age groups, the risk of people surviving into states of activity restriction and therefore its prevalence may well increase. However, one caveat to the pattern observed in disability-free life expectancy is the change to survey questions used to classify disability. A report on Measuring Disability in the Labour Force Survey (LFS), published by us in 2016, provides an overview of the likely impact of survey question changes on prevalence of disability suggested the introduction of new harmonised questions onto the LFS in April 2013 was on balance to reduce disability prevalence among those of working age.
Back to table of contents5. Health state life expectancies differ up to 3 years between UK countries
When looking at lower geography healthy and disability-free life expectancy it is important to note that sample sizes differ across areas, with Northern Ireland tending to have a smaller sample size than other countries.
Table 1: Healthy life expectancy at birth and age 65 across the UK, males, 2013 to 2015
| Life Expectancy (years) | Healthy Life Expectancy (years) | Proportion of LE (%) | Disability-free Life Expectancy (years) | Proportion of LE (%) | |
| At Birth | |||||
| United Kingdom | 79.2 | 63.1 | 79.7 | 62.7 | 79.2 |
| England | 79.5 | 63.4 | 79.8 | 63.0 | 79.3 |
| Wales | 78.4 | 61.5 | 78.4 | 60.0 | 76.5 |
| Scotland | 77.1 | 61.8 | 80.2 | 61.2 | 79.4 |
| Northern Ireland | 78.3 | 61.5 | 78.5 | 61.4 | 78.4 |
| At 65 | |||||
| United Kingdom | 18.5 | 10.3 | 55.9 | 9.9 | 53.3 |
| England | 18.7 | 10.5 | 56.0 | 10.0 | 53.4 |
| Wales | 18.1 | 9.8 | 54.0 | 8.7 | 48.1 |
| Scotland | 17.3 | 9.8 | 56.5 | 9.3 | 53.7 |
| Northern Ireland | 18.2 | 9.8 | 54.1 | 9.9 | 54.3 |
| Source: Office for National Statistics | |||||
Download this table Table 1: Healthy life expectancy at birth and age 65 across the UK, males, 2013 to 2015
.xls (27.6 kB)Males in Scotland have the lowest life expectancy at birth (77.1 years) and at age 65 (17.3 years) across the UK, but they report the highest proportion of life in good health at both ages (80.2% at birth, 56.5% at age 65) and disability-free at birth (79.4%). This suggests that surviving into states of ill health and dependency is lower in Scotland as limiting illness and dependency are most common in the oldest old. Males in England have the highest life expectancy at birth and at age 65 (79.5 and 18.7 years respectively) and the highest number of years spent in good health (63.4 and 10.5 years) or disability-free (63.0 and 10.0 years), they have the second highest proportion in good health and disability-free at birth and proportion in good health at age 65. Looking at healthy life expectancy, Wales and Northern Ireland spend on average the same amount of years in good health at birth which equates to a higher proportion in good health for Northern Ireland because of its lower life expectancy estimate. At age 65, Wales, Scotland and Northern Ireland men all spend on average 9.8 years in good health. Men in Wales can expect to spend less than half of their remaining life expectancy disability-free at age 65.
For each country, the proportion spent disability-free is lower than the proportion spent in good health apart from Northern Ireland at age 65. Northern Ireland has the highest proportion of remaining life spent disability-free.
Table 2: Healthy life expectancy at birth and age 65 across the UK, females, 2013 to 2015
| Life Expectancy (years) | Healthy Life Expectancy (years) | Proportion of LE (%) | Disability-free Life Expectancy (years) | Proportion of LE (%) | |
| At Birth | |||||
| United Kingdom | 82.9 | 63.9 | 77.1 | 62.4 | 75.3 |
| England | 83.1 | 64.1 | 77.1 | 62.6 | 75.4 |
| Wales | 82.3 | 62.7 | 76.2 | 59.6 | 72.4 |
| Scotland | 81.1 | 62.8 | 77.3 | 61.4 | 75.6 |
| Northern Ireland | 82.3 | 62.0 | 75.3 | 62.5 | 75.9 |
| At 65 | |||||
| United Kingdom | 20.9 | 11.1 | 53.1 | 10.1 | 48.4 |
| England | 21.1 | 11.2 | 53.2 | 10.2 | 48.5 |
| Wales | 20.5 | 10.7 | 52.3 | 9.0 | 44.1 |
| Scotland | 19.7 | 10.9 | 55.4 | 9.7 | 49.2 |
| Northern Ireland | 20.6 | 9.8 | 47.4 | 9.8 | 47.4 |
| Source: Office for National Statistics | |||||
Download this table Table 2: Healthy life expectancy at birth and age 65 across the UK, females, 2013 to 2015
.xls (27.6 kB)Females have higher life expectancy at birth than males and spend more years in good health, but spend a lower proportion of their lives in good health. The same can be seen at age 65 with the exception of Northern Ireland where both genders can expect to live the same amount of years in good health.
Females in England at birth and at age 65 have the highest life expectancy (83.1 and 21.1 years), healthy life expectancy (64.1 and 11.2 years) and disability-free life expectancy (62.6 and 10.2 years) estimates. At birth, females in Scotland have the highest proportion of life spent in good health (77.3%) and Northern Ireland have the highest proportion of life spent disability-free (75.9%). At age 65, Scotland has the highest proportion of remaining life spent in good health with 55.4% and disability-free with 49.2%.
For females in England, Wales and Scotland the proportion of life spent in good health is greater than that spent disability-free. At age 65 each country spends less than half of their remaining lives disability-free. In Northern Ireland, females at birth could expect to live a higher proportion of life disability-free, and at age 65 females could expect to live as many years in good health as disability-free.
Disability-free life expectancy was statistically significantly lower than healthy life expectancy at both birth and age 65 for males and females in the UK, England, Wales and for females in Scotland. For males in Scotland and both genders in Northern Ireland, there was no statistically significant differences between healthy and disability-free life expectancy.
Back to table of contents6. Health state life expectancies at birth differ by up to 19.6 years within countries
This is the first release (apart from when using the census) that encompasses sub-national areas across the UK for both life expectancy and health expectancies. As such it allows all sub-national areas to compare themselves to a UK average for the first time. However, health state life expectancy comparisons prior to 2013 to 2015 are only currently possible for the UK, constituent countries and sub-national areas within England.
Care needs to be taken when comparing local areas as some areas may have a smaller sample size than others. Confidence Intervals are provided in the reference tables, which should be considered when making comparisons.
Table 3: Top and bottom health state life expectancies at birth in local areas in the UK, males, 2013 to 2015
| Rank | Life Expectancy | Rank | Healthy Life Expectancy | Rank | Disability free Life Expectancy | |||
| Top | ||||||||
| 1 | Kensington and Chelsea (E) | 1 | Rutland (E) | 1 | Rutland (E) | |||
| 2 | East Dorset (E) | 2 | Wokingham (E) | 2 | Windsor and Maidenhead (E) | |||
| 3 | Hart (E) | 3 | Buckinghamshire (E) | 3 | Kingston upon Thames (E) | |||
| 4 | Guildford (E) | 4 | Windsor and Maidenhead (E) | 4 | Richmond upon Thames (E) | |||
| 5 | Harrow (E) | 5 | Harrow (E) | 5 | Wokingham (E) | |||
| Bottom | ||||||||
| 385 | North Lanarkshire (S) | 211 | Glasgow City (S) | 211 | Hartlepool (E) | |||
| 386 | Dundee City (S) | 212 | Manchester (E) | 212 | Caerphilly (W) | |||
| 387 | West Dunbartonshire (S) | 213 | Blaenau Gwent (W) | 213 | Tower Hamlets (E) | |||
| 388 | Blackpool (E) | 214 | Tower Hamlets (E) | 214 | Belfast (NI) | |||
| 389 | Glasgow City (S) | 215 | Causeway Coast and Glens (NI) | 215 | Blaenau Gwent (W) | |||
| Source: Office for National Statistics | ||||||||
| Notes: | ||||||||
| 1. (E) = England, (W) = Wales, (S) = Scotland, (NI) = Northern Ireland | ||||||||
| 2. Life Expectancy estimates for England are based on lower tier local authorities, Healthy and Disability-free life expectancy estimates are based on Upper Tier Local Authorities. | ||||||||
| 3. Local areas are Local Authorities in Wales, Council Areas in Scotland and Local Government District in Northern Ireland. | ||||||||
Download this table Table 3: Top and bottom health state life expectancies at birth in local areas in the UK, males, 2013 to 2015
.xls (29.2 kB)For Males at birth, all of the areas with highest health state life expectancy are in England. For the lowest areas there is more of a distribution across the four countries of the United Kingdom. For life expectancy, the majority of the lowest areas are from Scotland, but these change when looking at health and disability-free life expectancy.
A spreadsheet with all local area estimates across the UK can be found in the accompanying reference tables. Confidence intervals are provided alongside life expectancy estimates. If the confidence intervals of two different areas or time periods overlap then we cannot say that the difference is “statistically significant”. For this reason, care needs to be taken when comparing ranks of different areas.
Table 4: Top and bottom health state life expectancies at birth, countries in the UK, males, 2013 to 2015
| Country | Area | Life Expectancy | Area | Healthy Life Expectancy | Area | Disability-free Life Expectancy | ||
| Highest | ||||||||
| England | Kensington and Chelsea | 83.4 | Rutland | 71.1 | Rutland | 70.8 | ||
| Wales | Monmouthshire | 80.7 | Monmouthshire | 66.5 | Monmouthshire | 64.5 | ||
| Scotland | East Dunbartonshire | 80.5 | Perth and Kinross | 66.7 | Shetland Islands | 67.8 | ||
| Northern Ireland | Lisburn and Castlereagh | 79.9 | Lisburn and Castlereagh | 68.5 | Fermanagh and Omagh | 62.1 | ||
| Lowest | ||||||||
| England | Blackpool | 74.3 | Tower Hamlets | 54.0 | Tower Hamlets | 54.0 | ||
| Wales | Blaenau Gwent | 76.5 | Blaenau Gwent | 55.0 | Blaenau Gwent | 51.3 | ||
| Scotland | Glasgow City | 73.4 | Glasgow City | 55.9 | Glasgow City | 55.5 | ||
| Northern Ireland | Belfast | 75.9 | Causeway Coast and Glens | 54.0 | Belfast | 51.8 | ||
| Difference between highest and lowest areas | ||||||||
| England | 9.1 | 17.1 | 16.9 | |||||
| Wales | 4.2 | 11.5 | 13.2 | |||||
| Scotland | 7.1 | 10.8 | 12.2 | |||||
| Northern Ireland | 4.0 | 14.5 | 10.4 | |||||
| Source: Office for National Statistics | ||||||||
| Notes: | ||||||||
| 1. Life Expectancy estimates for England are based on lower tier local authorities, Healthy and Disability-free life expectancy estimates are based on Upper Tier Local Authorities. | ||||||||
| 2. Local areas are Local Authorities in Wales, Council Areas in Scotland and Local Government District in Northern Ireland. | ||||||||
| 3. Areas with small populations (such as Shetland Islands) tend to have wider confidence intervals than areas with larger populations. | ||||||||
Download this table Table 4: Top and bottom health state life expectancies at birth, countries in the UK, males, 2013 to 2015
.xls (29.7 kB)The smallest gap between a country’s highest and lowest life expectancy estimate is within Northern Ireland with 4.0 years difference. The biggest is over double this at 9.1 years in England, this is due to a higher estimate for life expectancy for the top area in England compared to the other constituent countries. The differences widen when looking at healthy life expectancy and disability-free life expectancy. For Northern Ireland the difference in years spent disability-free (10.6 years) is over double that of life expectancy and over three times as wide for years spend in good health (14.5 years). The smallest difference in healthy and disability-free life expectancy is in Scotland (10.8 and 12.2 years respectively), the largest is in England with 17.1 and 16.9 years respective difference between the highest and the lowest area.
Table 5: Top and bottom health state life expectancies at birth across the UK, females, 2013 to 2015
| Rank | Life Expectancy | Rank | Healthy Life Expectancy | Rank | Disability free Life Expectancy | |||
| Top | ||||||||
| 1 | Hart (E) | 1 | Orkney Islands (S) | 1 | Wokingham (E) | |||
| 2 | Kensington and Chelsea (E) | 2 | Richmond upon Thames (E) | 2 | Windsor and Maidenhead (E) | |||
| 3 | Camden (E) | 3 | Fermanagh and Omagh (NI) | 3 | Orkney Islands (S) | |||
| 4 | Westminster (E) | 4 | Wokingham (E) | 4 | West Berkshire (E) | |||
| 5 | Harrow (E) | 5 | Rutland (E) | 5 | Shetland Islands (S) | |||
| Bottom | ||||||||
| 385 | North Lanarkshire (S) | 211 | Kingston upon Hull, City of (E) | 211 | Hackney (E) | |||
| 386 | Blackpool (E) | 212 | Hartlepool (E) | 212 | Torfaen (W) | |||
| 387 | East Ayrshire (S) | 213 | Tower Hamlets (E) | 213 | Glasgow City (S) | |||
| 388 | Glasgow City (S) | 214 | Belfast (NI) | 214 | Tower Hamlets (E) | |||
| 389 | West Dunbartonshire (S) | 215 | Antrim and Newtownabbey (NI) | 215 | Antrim and Newtownabbey (NI) | |||
| Source: Office for National Statistics | ||||||||
| Notes: | ||||||||
| 1. (E) = England, (W) = Wales, (S) = Scotland, (NI) = Northern Ireland | ||||||||
| 2. Life Expectancy estimates for England are based on lower tier local authorities, Healthy and Disability-free life expectancy estimates are based on Upper Tier Local Authorities. | ||||||||
| 3. Local areas are Local Authorities in Wales, Council Areas in Scotland and Local Government District in Northern Ireland. | ||||||||
| 4. Areas with small populations (such as Orkney Islands) tend to have wider confidence intervals than areas with larger populations. | ||||||||
Download this table Table 5: Top and bottom health state life expectancies at birth across the UK, females, 2013 to 2015
.xls (29.7 kB)Females show a similar pattern as males, the top 5 life expectancies in the United Kingdom are in England and most of the bottom 5 is in Scotland. When looking at years spent in good health Orkney Islands (care should be taken due to small sample size and wide confidence intervals) in Scotland have the highest estimate and the third highest for years spent disability-free. Fermanagh and Omagh in Northern Ireland have the third highest estimate in healthy life expectancy.
When looking at the areas with the lowest estimates for health expectancies, we can see that these include areas from all four constituent countries.
Table 6: Top and bottom health state life expectancies at birth, countries in the UK, females, 2013 to 2015
| Country | Area | Life Expectancy | Area | Healthy Life Expectancy | Area | Disability-free Life Expectancy | ||
| Highest | ||||||||
| England | Hart | 86.7 | Richmond upon Thames | 71.1 | Wokingham | 71.8 | ||
| Wales | Monmouthshire | 84.1 | Gwynedd | 68.1 | Gwynedd | 64.3 | ||
| Scotland | East Dunbartonshire | 83.5 | Orkney Islands | 74.6 | Orkney Islands | 70.3 | ||
| Northern Ireland | Lisburn and Castlereagh | 83.3 | Fermanagh and Omagh | 71.0 | North Down and Ards | 63.7 | ||
| Lowest | ||||||||
| England | Blackpool | 79.4 | Tower Hamlets | 52.4 | Tower Hamlets | 53.5 | ||
| Wales | Merthyr Tydfil | 80.6 | Merthyr Tydfil | 56.2 | Torfaen | 54.7 | ||
| Scotland | West Dunbartonshire | 78.7 | North Ayrshire | 56.5 | Glasgow City | 54.1 | ||
| Northern Ireland | Belfast | 81.0 | Antrim and Newtownabbey | 47.8 | Antrim and Newtownabbey | 52.0 | ||
| Difference between highest and lowest areas | ||||||||
| England | 7.2 | 18.8 | 18.3 | |||||
| Wales | 3.5 | 11.9 | 9.6 | |||||
| Scotland | 4.8 | 18.1 | 16.2 | |||||
| Northern Ireland | 2.3 | 23.2 | 11.8 | |||||
| Source: Office for National Statistics | ||||||||
| Notes: | ||||||||
| 1. Life Expectancy estimates for England are based on lower tier local authorities, Healthy and Disability-free life expectancy estimates are based on Upper Tier Local Authorities. | ||||||||
| 2. Local areas are Local Authorities in Wales, Council Areas in Scotland and Local Government District in Northern Ireland. | ||||||||
| 3. Areas with small populations (such as Orkney Islands) tend to have wider confidence intervals than areas with larger populations. | ||||||||
Download this table Table 6: Top and bottom health state life expectancies at birth, countries in the UK, females, 2013 to 2015
.xls (29.7 kB)As can be seen in males, the gap in life expectancy between the highest and lowest estimates is smallest in Northern Ireland and largest in England. For Northern Ireland the gap in life expectancy (2.3 years) is almost half that of that seen in males. The gap for England was 7.2 years. The gap in healthy life expectancy and disability-free life expectancy between areas with countries was over double that for life expectancy. Even though Northern Ireland had the smallest life expectancy gap, it had the largest gap in healthy life expectancy (23.2 years), the largest gap in disability-free life expectancy was for England (18.3 years). The smallest gap in healthy and disability-free life expectancy can be seen in Wales, 11.9 and 9.6 years respectively.
Figure 3 highlights the differences between life expectancy in males and females across the UK.
Figure 3: Life expectancy (LE) at birth for males and females, by local area, UK, 2013 to 2015
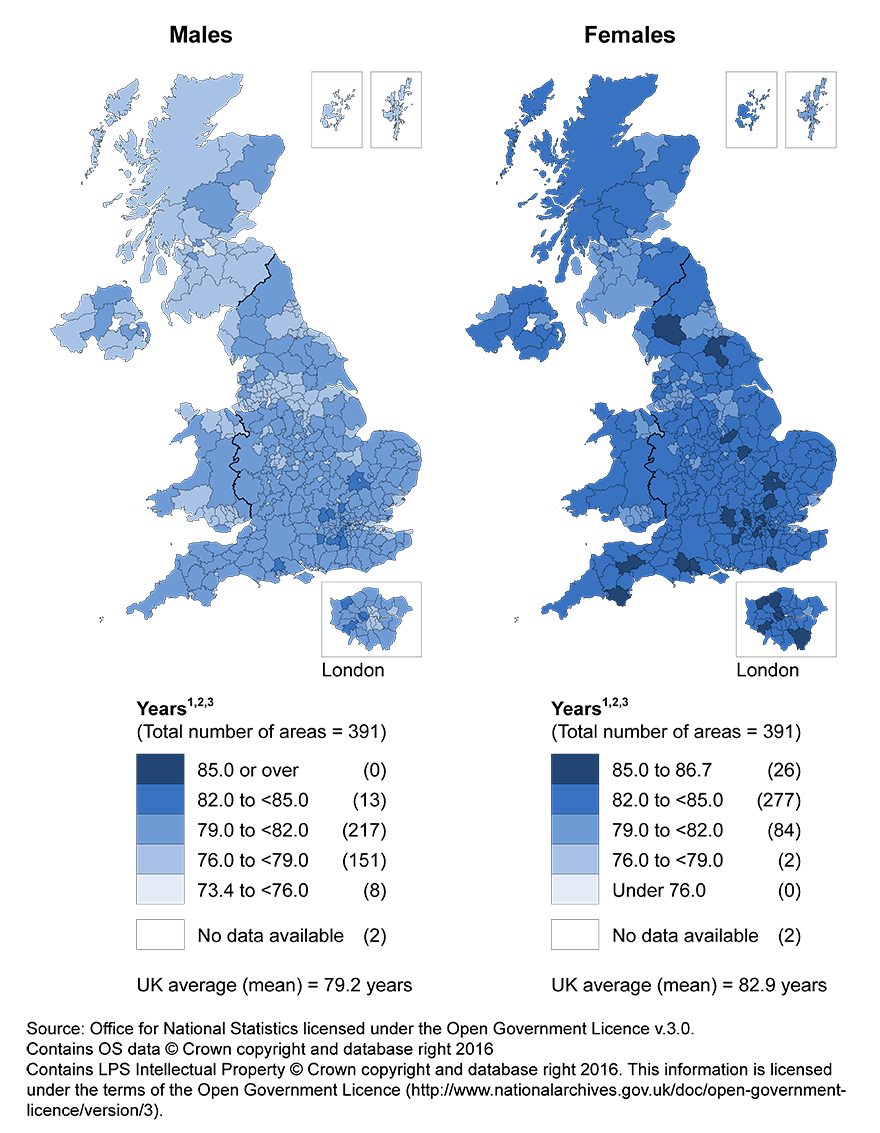
Notes:
- Local areas include lower tier local authorities (LTLAs) in England, unitary authorities in Wales, council areas in Scotland and local government districts in Northern Ireland.
- Isles of Scilly and City of London have been excluded from the map because of insufficient population counts.
Download this image Figure 3: Life expectancy (LE) at birth for males and females, by local area, UK, 2013 to 2015
.png (493.4 kB)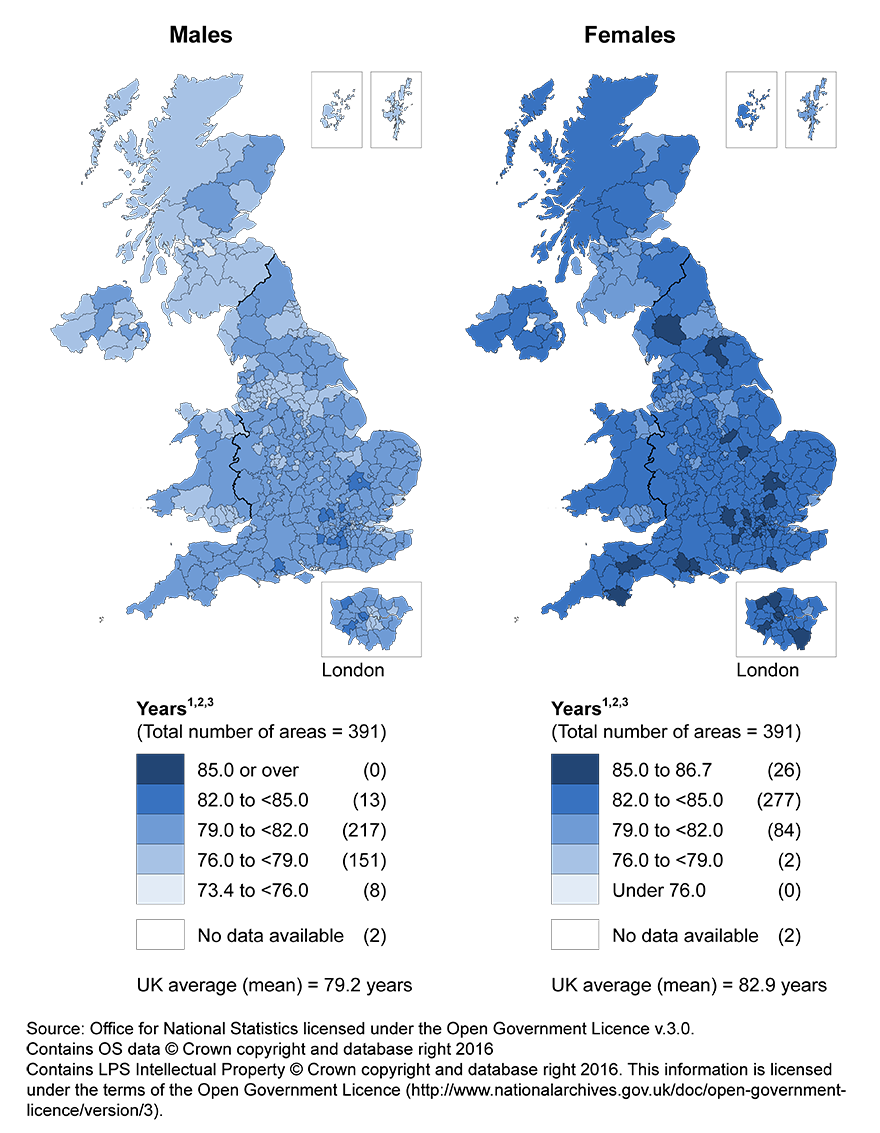{kind=link}
The maps show that for each area females are living longer than males. For males, there were 13 areas that had a life expectancy estimate of 82.0 years or over. In comparison, over three quarters of areas (303 areas) for females had a life expectancy estimate of 82.0 years or over. 40.7% of areas for males had an estimate of 79.0 years or lower, this was 0.5% of areas for females.
Back to table of contents7. Life expectancy at age 65 differ by up to 5.6 years within countries
Figure 4: Highest and lowest number of years expected to live for men and women at age 65, by local area, UK, 2013 to 2015
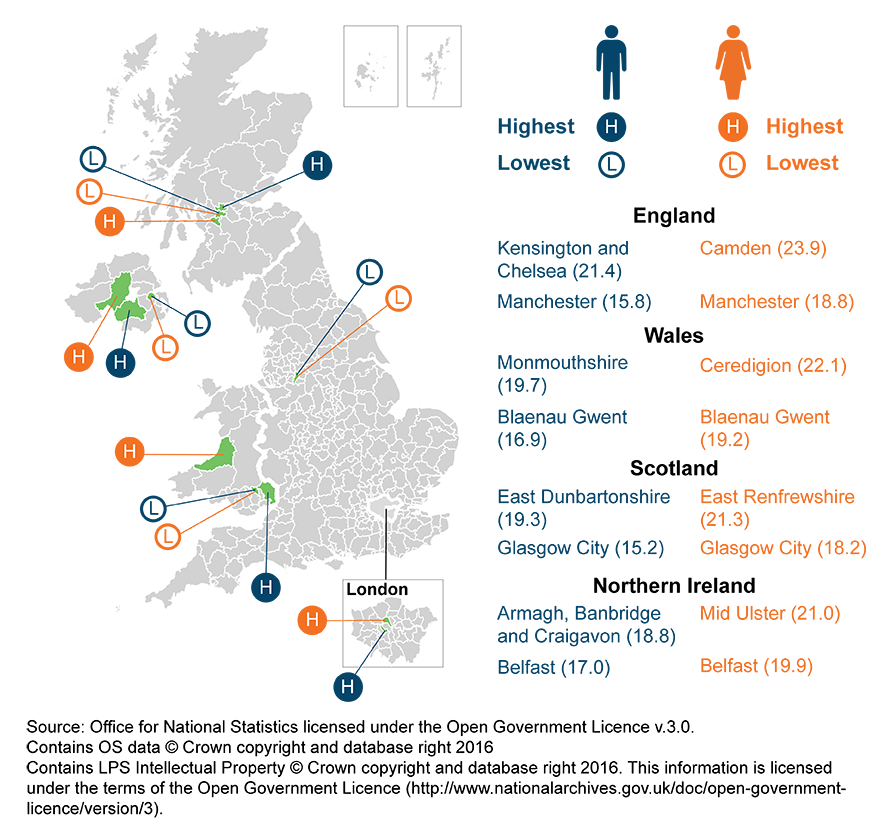
Notes:
- Local areas have been ranked at their country level to more than one decimal place.
- Local areas include lower tier local authorities in England, unitary authorities in Wales, council areas in Scotland and local government districts in Northern Ireland.
- Isles of Scilly and City of London have been excluded from the local area rankings because of insufficient population counts.
Download this image Figure 4: Highest and lowest number of years expected to live for men and women at age 65, by local area, UK, 2013 to 2015
.png (327.4 kB)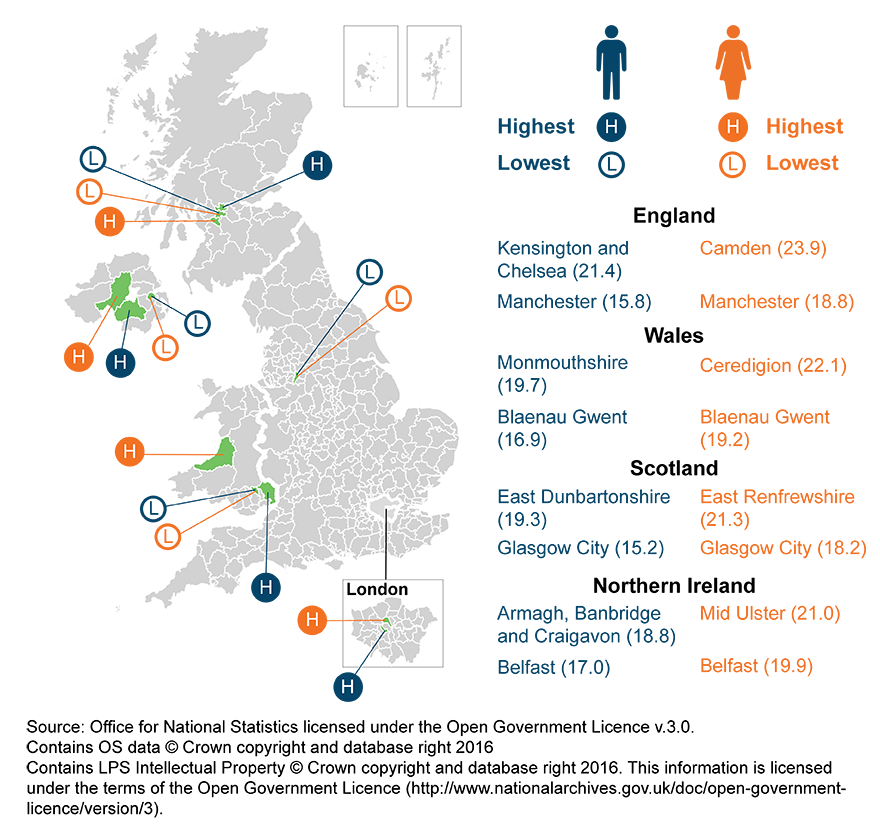{kind=link}
The majority of highest and lowest life expectancy in areas for males is the same at birth and at age 65. The exceptions are the highest life expectancy at age 65 for Northern Ireland being Armagh, Banbridge and Craigavon (which was Lisburn and Castlereagh at birth) and the lowest life expectancy for England at age 65 being Manchester (which was Blackpool at birth).
The opposite can be seen for females where the majority of highest and lowest life expectancies are different for each country. The only figure that was the same at birth and at age 65 was the lowest life expectancy in Northern Ireland, which was in Belfast.
Back to table of contents8. What are health expectancies?
Health expectancies add a quality of life dimension to estimates of life expectancy (LE) by dividing expected lifespan into time spent in different states of health or disability. Healthy life expectancy (HLE), which estimates lifetime spent in “Very good” or “Good” health, is based on how individuals perceive their general health. The second is disability-free life expectancy (DFLE), which estimates lifetime free from a limiting persistent illness or disability. This is based upon a self-rated assessment of how health conditions and illnesses limit an individual’s ability to carry out day-to-day activities. Both health expectancies are summary measures of population health and important indicators of the well-being of society, providing context to the impacts of policy changes and interventions at both national and local levels. Health expectancies are used across public, private and voluntary sectors, in the assessment of healthy ageing, fitness for work, monitoring health improvement, fairness in extensions to the state pension age, pension provision and health and social care need.
The 2013 to 2015 figures in this publication represent the expected life years in health states for an individual, assuming 2013 to 2015 mortality and health status rates apply throughout that individual’s life. Therefore, they provide a snapshot of the health status of the population(s) in the UK and its sub-national areas during 2013 to 2015. The health status and mortality rates of a population change year on year due to exposure to different risks and treatments affecting health, and also through inward and outward migration. Therefore, the estimates reported in this bulletin should not be interpreted as the actual number of years a person will live in different health states. HE figures are a likely estimate should the health status and mortality rates remain fairly stable over the life course.
Health state life expectancies are based on subjective self-reports using the following survey questions:
“How is your health in general; would you say it was...”
- Very good
- Good
- Fair
- Bad
- Very bad
If a respondent answered “Very good” or “Good” they were classified as having “Good” health. Those who answered “Fair”, “Bad”, or “Very bad” were classified as having “Not Good” health.
The disability questions are as follows:
Table 7: Changes to the disability questions in the Annual Population Survey from April 2013
| LFS QUESTIONS (before April 2013) | HARMONISED QUESTIONS (from April 2013) |
| LNGLIM | LNGLST (replacing LNGLIM) |
| Do you have any health problems or disabilities that you expect will last for more than a year? | Do you have any physical or mental health conditions or illnesses lasting or expected to last 12 months or more? |
| 1 Yes | 1 Yes |
| 2 No | 2 No |
| HEALIM | LIMACT (replacing HEALIM) |
| Do these health problems or disabilities, when taken singly or together, substantially limit your ability to carry out normal day-to-day activities? | Does your condition or illness/do any of your conditions or illnesses reduce your ability to carry out day-to-day activities? |
| 1 Yes | 1 Yes, a lot |
| 2 No | 2 Yes, a little |
| 3 Not at all | |
| Source: Office for National Statistics | |
| Notes: | |
| 1. LFS – Labour Force Survey | |
| 2. LNGLIM – variable name of question used in the LFS to capture whether the respondent self reports having a health problem or disability that has lasted for a year or more (discontinued April 2013) | |
| 3. LNGLST - variable name of question used in the LFS to capture self reports of activity limitation associated with the reporting of any health problems or conditions reported in LNGLIM (discontinued April 2013) | |
| 4. HEALIM - variable name of question used in the LFS to capture whether the respondent self reports any physical or mental health conditions or illnesses lasting a year or more (from April 2013) | |
| 5. LIMACT - variable name of question used in the LFS to capture self reports of activity limitation by extent (from April 2013) | |
Download this table Table 7: Changes to the disability questions in the Annual Population Survey from April 2013
.xls (28.7 kB)The questions classifying individuals to activity limitation where changed in 2013 following a review into how disability should be measured in national surveys. Primary harmonised standards for disability data collection and the production of statistical measures of disability are available on our website. This means that the survey data used in this release is predominantly based on the questions in column 2 which classified someone as having a disability if they answer yes LNGLST and answer “yes, a lot” or “yes, a little” to LIMACT. For column 1 they would be classified as disabled if they answered yes to both questions in column 1. One important difference between these questions is that LNGLST now explicitly mentions mental as well as physical conditions, designed to improve the capture of mental health conditions and illness. Due to this change and the change in the introductory paragraph of the disability section being reworded in 2010, there has been a difference in the number of people reporting disabilities. Therefore, estimates either side of the discontinuity (before and after April 2013) should not be directly compared.
Changes in health expectancies over time are assessed by comparing non-overlapping time periods. Therefore, estimates for 2013 to 2015 should not be compared with estimates for 2012 to 2014 or 2011 to 2013 for example, as they will contain some of the same survey respondents.
Back to table of contents9. How do we calculate health state life expectancies?
In this bulletin, data were calculated using abridged life table methods (based on 5-year age groups). Life expectancy (LE) has been calculated using the standard Chiang II abridged life table method. However, estimation of the variance, used to measure the statistical precision of life expectancy estimates, has undergone one important modification as the Chiang II method assumes zero variance for the final age group. To enable the calculation of a confidence interval for the final age band, the method developed by Silcocks et al (2001) has been used and further information is available in the methods paper published earlier this year. Separate tables were constructed for males and females using numbers of deaths registered and mid-year population estimates for 3 consecutive years.
Figures for England, Wales, regions, counties and local authorities exclude deaths of non-residents. However, Scotland includes non-usual residents who die in Scotland and do not have an area of residence within Scotland and imputation is used to assign to geography of “residence” (see section 1.3.1 in the following Healthy life expectancy: technical paper for more detail). Northern Ireland also includes non-usual residents whom are allocated to place of death (see Life Expectancy for Northern Ireland Information Paper & Methodology Guide for more detail).
The data used in calculating the general health and disability was obtained from the annual population survey (APS). It was aggregated over a 3-year period to achieve sufficiently large sample sizes to enable meaningful statistical comparison at national and sub-national level.
However, as the size of each upper tier local authority in England, local authority in Wales, Scottish council area and Northern Ireland local government districts varies, the number of respondents sampled in some areas was a lot smaller than for others. For these authorities with relatively small sample sizes, such as the London borough of Tower Hamlets, the estimates are more susceptible to large fluctuations because of the impact of random variation.
The prevalence of “Good” general health and disability-free among males and females resident in private households in England was compared across areas. HLE was then calculated using the Sullivan method, which combines prevalence data with mortality and mid-year population estimates (MYPE) over the same period and geographical coverage to calculate estimates of life expectancy (LE) and healthy life expectancy (HLE) by age and sex (ONS Life Table Template, Jagger et al., (2014).
The APS provides prevalence information for those aged 16 years and over. We are able to estimate lower age groups by using a census imputation method.
Results are presented with 95% confidence intervals in reference tables to help interpretation. Confidence intervals in this statistical bulletin indicate the uncertainty surrounding HE estimates and allow more meaningful comparisons between areas. Within this bulletin, a difference which is described as “significant” is statistically significant and has been assessed using 95% confidence intervals.
Back to table of contents10. How do constituent countries health expectancies compare to other estimates?
National life tables (NLT) are period life expectancy estimates. Figures calculated in this analysis are cohort life expectancy estimates. NLT are produced for 3-year aggregated periods for the UK and constituent countries and estimates may differ to those produced in this analysis. Due to the differences in life expectancy methods, numbers in this publication are incomparable to those in the NLT.
We produced estimates across lower geographies in the UK in October 2016. These estimates used a different source (2011 Census) and had data available for all ages, so adjustment was not needed. Therefore these estimates are not comparable to those published in this bulletin.
Figures in Wales are published using the 85 and over final age group and 5-year aggregated period. The latest release uses the Welsh health survey. Public Health Wales figures are also calculated using a different question on general health and disability.
Figures in Scotland are published using the 85 and over final age group and 5-year aggregated period based on the Scotland 2011 census for health prevalence. Estimates are also produced at single year at the Scotland level.
Figures in Northern Ireland are published using the 85 and over final age group and 3-year aggregated periods. It is published for Northern Ireland country level, quintiles and urban or rural. Estimates are produced using the Health Survey Northern Ireland.
Back to table of contents11. Quality and Information
The Health Expectancies Quality and Methodology Information document contains important information on:
- the strengths and limitations of the data
- the quality of the output: including the accuracy of the data, how it compares with related data
- uses and users
- how the output was created