1. Main points
Provisional analysis for the period 2 March to 15 May 2020 shows, that after taking into account size and age structure of the population, the mortality rate for deaths involving COVID-19 was highest among males of Black ethnic background at 255.7 deaths per 100,000 population and lowest among males of White ethnic background at 87.0 deaths per 100,000.
For females, the pattern was similar with the highest rates among those of Black ethnic background (119.8) and lowest among those of White ethnic background (52.0).
To understand and explain these differences we explored further with statistical modelling using information from only private households included in the 2011 Census.
This analysis showed that for all ages the rate of deaths involving COVID-19 for Black males was 3.3 times greater than that for White males of the same age, while the rate for Black females was 2.4 times greater than for White females.
After adjusting for region, population density, socio-demographic and household characteristics, the raised risk of death involving COVID-19 for people of Black ethnic background of all ages together was 2.0 times greater for males and 1.4 times greater for females compared with those of White ethnic background.
Males of Bangladeshi, Pakistani and Indian ethnic background also had a significantly higher risk of death involving COVID-19 (1.5 and 1.6 times, respectively) than White males once region, population density, socio-demographic and household characteristics were accounted for; whilst for females in Bangladeshi or Pakistani, Indian, Chinese and Mixed ethnic groups the risk of death involving COVID-19 was equivalent to White females.
When looking at total number of deaths involving COVID-19 88.6% were of people from a White ethnic group, 6.2 % from an Asian ethnic group, 4.0% from a Black ethnic group and 0.5 % from an Other ethnic group.
Our research was based on linking deaths to the 2011 census, the most timely data available, including people aged 9 years and over; we used a regression model to adjust for specific characteristics for people in private households at the time of the 2011 Census, and we aim to undertake further analysis that takes into account other characteristics such as pre-existing conditions in future projects.
Statistician's comments
“ONS analysis continues to show that people from a Black ethnic background are at a greater risk of death involving COVID-19 than all other ethnic groups. The risk for black males has been more than three times higher than white males and nearly two and a half times higher for black females than white. Adjusting for socio-economic factors and geographical location partly explains the increased risk, but there remains twice the risk for Black males and around one and a half times for black females. Significant differences also remain for Bangladeshi, Pakistani and Indian men. The ONS will continue to research this unexplained increased risk of death, examining the impact of other health conditions.”
Nick Stripe, Head of Life Events, Office for National Statistics
Back to table of contents2. Introduction
This article presents provisional analyses of deaths involving the coronavirus (COVID-19) by ethnic group for England and Wales. It includes deaths involving COVID-19 that occurred between 2 March and 15 May 2020, registered by 29 May 2020. Ethnic group is not recorded on the death certificate; to enable us to undertake these analyses, death registrations up to 29 May 2020 have been linked to the 2011 Census, which allowed us to ascertain the self-reported ethnicity of the deceased and other demographic factors. Analyses have been restricted to those aged nine years and over because children aged under nine years would not have been born and therefore included in the 2011 Census. More details on the data used can be found in the technical appendix.
Embed code
The breakdown of ethnic group we used in this article was guided by the number of deaths available for analyses, following the data linkage, and the distribution across ethnic groups. We have therefore had to combine certain ethnic groups together to ensure we can provide robust statistical analysis. Table 1 shows the breakdown of ethnic groups primarily used in this article. However, a more detailed breakdown is shown in Tables 2 and 3, which present counts of deaths involving COVID-19 by ethnic group for the study period analysed in this article.
| Ethnic groups used | Detailed composition of groups | |
|---|---|---|
| White | White British; Irish; Gypsy or Irish Traveller; Other White | |
| Mixed/Multiple Ethnic Groups | White and Black Caribbean; White and Asian; White and Black African; Other Mixed | |
| Indian | Indian | |
| Bangladeshi\Pakistani | Bangladeshi\Pakistani | |
| Chinese | Chinese | |
| Black | Black Caribbean; Black African; Black Other | |
| Other Ethnic group | Asian other; Arab; Other ethnic group |
Download this table Table 1: Ethnic breakdowns used in this article
.xls .csv3. Ethnic group breakdown of COVID-19 deaths by age and sex
Table 2 shows the number of deaths involving the coronavirus (COVID-19) and their percentage distribution across the fully expanded ethnic group classification among the study population. We report deaths for England and Wales, including deaths outside of hospital, and include both confirmed and suspected cases. A separate table containing deaths by ethnic group occurring in Wales is provided in the datasets accompanying this release.
Of the deaths involving COVID-19 that occurred between 2 March and 15 May 2020, 88.6% were among those of White ethnic background. Those of Indian ethnic background comprised 2.7% and those of Black Caribbean ethnic background 2.4% of deaths involving COVID-19.
| Ethnic group | COVID-19 deaths | Percentage of COVID-19 deaths | |
|---|---|---|---|
| White | 33,630 | 88.6 | |
| English/Welsh/Scottish/Northern Irish/British | 32,160 | 84.7 | |
| Irish | 666 | 1.8 | |
| Gypsy or Irish Traveller | 16 | 0.0 | |
| Other White | 788 | 2.1 | |
| Mixed/Multiple ethnic groups | 252 | 0.7 | |
| White and Black Caribbean | 86 | 0.2 | |
| White and Black African | 31 | 0.1 | |
| White and Asian | 53 | 0.1 | |
| Other Mixed | 82 | 0.2 | |
| Asian /Asian British | 2,355 | 6.2 | |
| Indian | 1,011 | 2.7 | |
| Pakistani | 551 | 1.5 | |
| Bangladeshi | 222 | 0.6 | |
| Chinese | 137 | 0.4 | |
| Other Asian | 434 | 1.1 | |
| Black/African/Caribbean/Black British | 1,513 | 4.0 | |
| African | 481 | 1.3 | |
| Caribbean | 911 | 2.4 | |
| Other Black | 121 | 0.3 | |
| Other ethnic group | 206 | 0.5 | |
| Arab | 63 | 0.2 | |
| Other Ethnic Group | 143 | 0.4 | |
| Total | 37,956 | 100.0 | |
Download this table Table 2: Number and percentage of deaths involving COVID-19 by ethnic group, England and Wales, deaths occurring between 2 March and 15 May 2020
.xls .csvThe populations we used in these analyses are shown in Table 3. Those of White British ethnic group constituted more than four-fifths of the population investigated. With the White ethnic group as a whole making 86.4% of the total.
| Ethnic group | Percentage | |
|---|---|---|
| English/Welsh/Scottish/Northern Irish/British | 80.9 | |
| Irish | 0.9 | |
| Gypsy or Irish Traveller | 0.1 | |
| Other White | 4.5 | |
| White and Black Caribbean | 0.7 | |
| White and Black African | 0.3 | |
| White and Asian | 0.6 | |
| Other Mixed | 0.5 | |
| Indian | 2.6 | |
| Pakistani | 2.1 | |
| Bangladeshi | 0.8 | |
| Chinese | 0.6 | |
| Other Asian | 1.4 | |
| African | 1.7 | |
| Caribbean | 1.1 | |
| Other Black | 0.4 | |
| Arab | 0.3 | |
| Other Ethnic Group | 0.5 | |
| Total | 100.0 |
Download this table Table 3: Weighted populations at 2 March 2020 used in this article, by ethnic group
.xls .csvBreaking the deaths down further by age and sex, we see that deaths involving COVID-19 are more numerous for males in all ethnic groups other than "White and Black Caribbean" and "Other Mixed" ethnic groups at younger ages and in people aged 65 years and over compared with those under 65 years for all ethnic groups (Table 4).
| Ethnic Group | Males | Females | |||
|---|---|---|---|---|---|
| Ages 9 to 64 years | Aged 65 years and above | Ages 9 to 64 years | Aged 65 years and above | ||
| White | 1,619 | 16,715 | 979 | 14,317 | |
| English/Welsh/Scottish/ Northern Irish/British | 1,509 | 16,008 | 938 | 13,705 | |
| Irish | 20 | 338 | 8 | 300 | |
| Gypsy or Irish Traveller | 3 | 7 | 0 | 6 | |
| Other White | 87 | 362 | 33 | 306 | |
| Mixed/Multiple ethnic group | 23 | 125 | 24 | 80 | |
| White and Black Caribbean | 8 | 45 | 9 | 24 | |
| White and Black African | 4 | 16 | 2 | 9 | |
| White and Asian | 5 | 28 | 3 | 17 | |
| Other Mixed | 6 | 36 | 10 | 30 | |
| Asian/Asian British | 426 | 1,064 | 199 | 666 | |
| Indian | 159 | 472 | 70 | 310 | |
| Pakistani | 103 | 246 | 68 | 134 | |
| Bangladeshi | 57 | 101 | 14 | 50 | |
| Chinese | 14 | 70 | 6 | 47 | |
| Other Asian | 93 | 175 | 41 | 125 | |
| Black/African/ Caribbean/Black British | 260 | 678 | 161 | 414 | |
| African | 139 | 173 | 78 | 91 | |
| Caribbean | 87 | 468 | 64 | 292 | |
| Other Black | 34 | 37 | 19 | 31 | |
| Other ethnic group | 40 | 106 | 14 | 46 | |
| Arab | 14 | 35 | 4 | 10 | |
| Other Ethnic Group | 26 | 71 | 10 | 36 | |
| Total | 2,368 | 18,688 | 1,377 | 15,523 | |
Download this table Table 4: Number of deaths involving COVID-19 by age, sex and ethnic group, England and Wales, deaths occurring between 2 March and 15 May 2020
.xls .csv4. Age-standardised mortality rates of death involving COVID-19 by ethnic group
We calculated age-standardised mortality rates (ASMRs)1 for males and females aged nine years and over, aged 9 to 64 years, and aged 65 years and over to assess when contrasts were different among younger and older populations. ASMRs of death involving the coronavirus (COVID-19) can be interpreted as deaths per 100,000 of the population during the analysis period.
Table 5 shows ASMRs for deaths involving COVID-19 among males and females aged 9 years and over per 100,000 of the population at risk. Figures 1 and 2 show the patterns by sex and ethnic group among those aged 9 to 64 years and 65 years and over respectively.
| Ethnic group | Males | Females | ||||
|---|---|---|---|---|---|---|
| Rate | Lower 95% confidence limit | Upper 95% confidence limit | Rate | Lower 95% confidence limit | Upper 95% confidence limit | |
| Bangladeshi and Pakistani | 191.0* | 172.9 | 209.1 | 100.8* | 87.9 | 113.7 |
| Black | 255.7* | 238.1 | 273.3 | 119.8* | 109.5 | 130.1 |
| Chinese | 119.5* | 94.2 | 149.2 | 65.4 | 48.4 | 86.3 |
| Indian | 157.6* | 144.8 | 170.3 | 86.8* | 77.9 | 95.6 |
| Mixed | 144.4* | 120.4 | 168.5 | 75.9* | 60.5 | 91.3 |
| Other | 167.7* | 150.1 | 185.3 | 83.4* | 72.0 | 94.8 |
| White | 87.0 | 85.8 | 88.3 | 52.0 | 51.1 | 52.8 |
Download this table Table 5: Age-standardised mortality rates for deaths involving COVID-19 with 95% confidence intervals by sex and ethnic group, per 100,000 people, England and Wales, deaths occurring between 2 March and 15 May 2020
.xls .csvMales of Black ethnic background aged nine years and over had a statistically significantly higher ASMR of death involving COVID-19 than males of other ethnic backgrounds, at 255.7 deaths per 100,000 population (Table 5). Their rate of death was 2.9 times greater than those of the White males, which reflects a lessening in the comparative risk found in our previous publication where the age-adjusted risk was 4.2 times greater in the measurement of deaths occurring between 2 March and 10 April 2020. This suggests the gap has narrowed following the inclusion of more recent deaths up to 15 May 2020.
There were also notably raised rates of death among males in the Bangladeshi or Pakistani, Indian, and Other ethnic group males; men in these ethic groups have rates 2.2 times, 1.8 times and 1.9 times higher than males of the White ethnic group, respectively. In fact, White males had a statistically significantly lower rate of death involving COVID-19 than all other ethnic groups (Table 5).
Females had a lower rate of death involving COVID-19 than males across all ethnic groups, with Black females having less than half the rate of Black males. However, Black females had a statistically significantly higher rate than White males despite males generally being at greater risk.
The pattern for females was largely like that of males. Females of Black ethnic background had the highest rate of death involving COVID-19, at 119.8 deaths per 100,000, 2.3 times higher than White females. All other ethnic groups, other than Chinese, had a statistically significantly raised rate of death compared with White females.
ASMR of death by ethnic group with 95% confidence intervals for other age groups are available in the datasets accompanying this release.
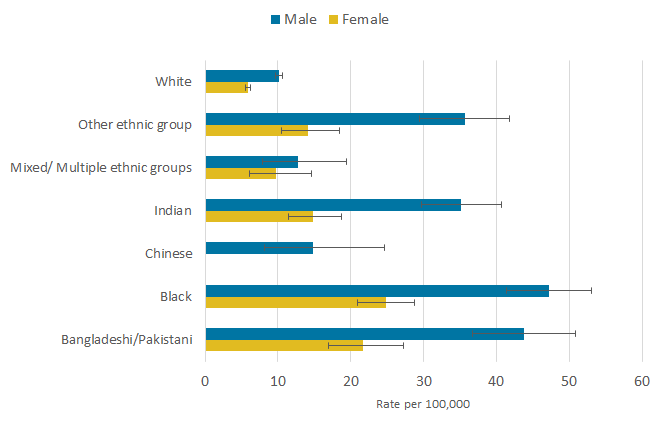
When mortality rates are isolated to younger males aged 9 to 64 years, the relative differences are larger. Males of Black ethnic background had a statistically significantly higher ASMR of death involving COVID-19 than males from Mixed, Chinese and White ethnic backgrounds, standing at 47.3 deaths per 100,000 population (Figure 1). Their rate of death was 4.7 times greater than those of White males, which shows relative risk is somewhat higher among a younger demographic, notwithstanding rates are based on a smaller number of deaths (Table 4).
Males aged 9 to 64 years of Bangladeshi or Pakistani ethnic background also had a 4.3 times significantly higher rate of death than White males; statistically significantly higher rates of deaths were also observed among males of Indian and Other ethnic groups compared with White males (Figure 1).
Figure 1: Males of Black ethnic background, aged between 9 and 64 years of age, had a rate of death 4.7 times higher than those of White ethnic background in England and Wales
Age-standardised rates for deaths involving COVID-19 at ages 9 to 64 years by sex and ethnic group, per 100,000 people: England and Wales, occurring 2 May to 15 May 2020
Source: Office for National Statistics
Notes:
- Office for National Statistics (ONS) figures based on death registrations up to 29 May 2020 that occurred between 2 March and 15 May 2020 that could be linked to the 2011 Census for the coronavirus (COVID-19) rate of death.
- Deaths were defined using the International Classification of Diseases, 10th Revision (ICD-10). Deaths involving COVID-19 include those with an underlying cause, or any mention, of ICD-10 codes U07.1 (COVID-19, virus identified) or U07.2 (COVID-19, virus not identified).
- Age-standardised mortality rates (ASMRs) of death involving COVID-19 can be interpreted as deaths per 100,000 of the population during the period at risk.
- Other ethnic group encompasses Asian other, Arab and other ethnic group categories in the classification.
- Non-overlapping error bars denote a statistically significant difference in rates of death.
- Because of low counts, the rates for Chinese females are deemed unreliable; therefore, we could not calculate confidence intervals around their estimate.
Download this image Figure 1: Males of Black ethnic background, aged between 9 and 64 years of age, had a rate of death 4.7 times higher than those of White ethnic background in England and Wales
.png (11.4 kB) .xlsx (29.1 kB)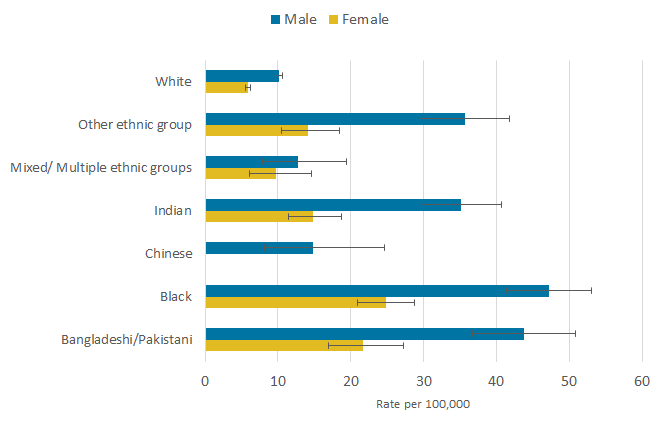{kind=link}
For females, those from a Black ethnic background had the highest rate for deaths involving COVID-19, at 24.8 deaths per 100,000; the relative gap was 4.2 times higher among those of Black females compared with White females. Females of Bangladeshi or Pakistani ethnic background had a rate of death that was 3.7 times higher than that of White females. Females of White ethnic background had a statistically significantly lower rate of death compared with females of Black, Bangladeshi or Pakistani, Indian, and Other ethnic backgrounds.
At ages 65 years and over, men of Black ethnic background had a statistically significantly higher rate of death involving COVID-19 than all other ethnic groups (Figure 2), at 1015.8 deaths per 100,000 population2 and 2.8 times higher than those of White ethnic background, whose rate was the lowest. Bangladeshi or Pakistani men had a rate of death twice that of White men.
Women of Black ethnic background also had the highest rate of death, 2.1 times higher than White women, who had the lowest rate (Figure 2). Women with an ethnic background other than Chinese had a statistically significantly higher rate of death involving COVID-19 than that of White women.
Figure 2: Females of Black ethnic background aged 65 years and over had a rate of death 2.1 times higher than that of White females
Age-standardised mortality rates for deaths involving COVID-19 at ages 65 years and over by sex and ethnic group, per 100,000 people, England and Wales, deaths occurring 2 March to 15 May 2020

Source: Office for National Statistics
Notes:
- Office for National Statistics (ONS) figures based on death registrations up to 29 May 2020 that occurred between 2 March and 15 May 2020 that could be linked to the 2011 Census for the coronavirus (COVID-19) rate of death.
- Deaths were defined using the International Classification of Diseases, 10th Revision (ICD-10). Deaths involving COVID-19 include those with an underlying cause, or any mention, of ICD-10 codes U07.1 (COVID-19, virus identified) or U07.2 (COVID-19, virus not identified).
- Age-standardised mortality rates (ASMRs) of death involving COVID-19 can be interpreted as deaths per 100,000 of the population during the period at risk.
- Other ethnic group encompasses Asian other, Arab and other ethnic group categories in the classification.
- Non-overlapping error bars denote a statistically significant difference in rates of death.
Download this image Figure 2: Females of Black ethnic background aged 65 years and over had a rate of death 2.1 times higher than that of White females
.png (12.1 kB) .xlsx (29.0 kB)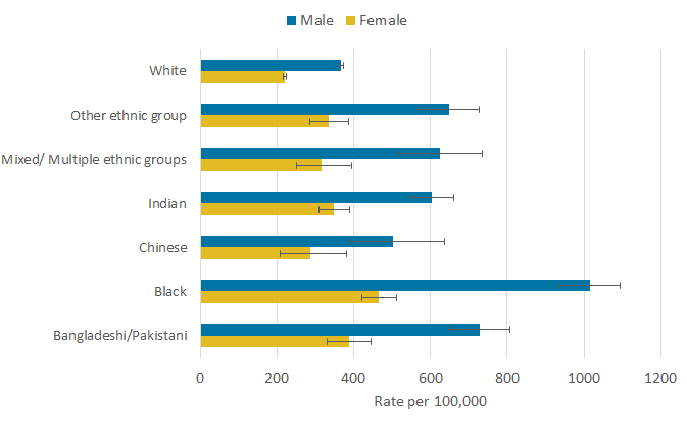{kind=link}
Based on these figures, those from a Black ethnic background appear particularly vulnerable to mortality involving COVID-19, as do other minority ethnic groups to differing extents. When assessing these results, it is important to take account of whether the differences observed in risk of dying across ethnic groups is correlated with geographic and socio-economic factors such as deprivation. The following section explores how much variation in risk can be accounted for by some of the social determinants of health available from the 2011 Census.
Notes for: Age-standardised rates of death involving COVID-19 by ethnic group
ASMRs enable populations with different age structures to be compared validly. Those of White ethnic background have an older population structure to other ethnic groups, and as COVID-19 deaths are more common in older populations, it is necessary to adjust for population structure.
The population of males of Black ethnicity in the study population was 61,742; therefore, this is the number of deaths we would have expected to have observed had the population been 100,000. This equates to 10.15 deaths per 1000, a death rate of approximately 1%.
5. Ethnic group differences in deaths involving COVID-19, adjusted for socio-demographic factors
Differences in the risk of death involving the coronavirus (COVID-19) may be driven by factors related to the risk of being infected, susceptibility to more severe outcomes once infected and ability to survive once infected by the virus. Factors affecting the risk of infection are likely to include geographic location and population density, living arrangements, socio-economic profile, and working conditions. Differences in these characteristics, and what they may imply for current circumstances, may also be associated with the risk of death once infected. It is important to note that this analysis has been undertaken at the population level and will not relate to all people’s individual circumstance and backgrounds.
We used Cox proportional hazards regression models to estimate whether the risk of a death involving COVID-19 differs across ethnic groups, after adjusting for a wide range of geographic, demographic, socio-economic, living arrangement and exposure measures derived from the 2011 Census.1 The statistical models are explained in the technical appendix. These characteristics may help to explain the association between COVID-19 mortality and a person’s ethnic background, and they are important to adjust for to enable us to quantify the differences in the rate of death specifically associated with ethnic background.
The modelling analyses section is based on those that were enumerated in private households only at the 2011 Census, as only private household enumerations had the entirety of the socio-demographic and household characteristics used in the modelling of mortality risk. Therefore, this section excludes people enumerated in communal establishments at the 2011 Census.
Figure 3: How the risk of death involving COVID-19 varies by ethnic group for males and females relative to the White population
Rate of COVID-19 death by ethnic group and sex relative to the White population, England and Wales, 2 March to 15 May 2020
Embed code
Notes:
Cox proportional hazards models adjusting for age. Fully adjusted models also include region, population density, area deprivation, household composition, socio-economic position, highest qualification held, household tenure, multigenerational household flags and occupation indicators (including key workers and exposure to others) in 2011.
Office for National Statistics (ONS) figures based on death registrations up to 29 May 2020 that occurred between 2 March and 15 May 2020 that could be linked to the 2011 Census for the coronavirus (COVID-19) rate of death.
Deaths were defined using the International Classification of Diseases, 10th Revision (ICD-10). Deaths involving COVID-19 include those with an underlying cause, or any mention, of ICD-10 codes U07.1 (COVID-19, virus identified) or U07.2 (COVID-19, virus not identified).
Rate of death between 2 March and 15 May 2020.
Other ethnic group encompasses Asian other, Arab and other ethnic group categories in the classification.
Error bars not crossing the x-axis at value 1.0 denote a statistically significant difference in relative rates of death.
In Figure 3, we show how the rate of death involving COVID-19 varies by ethnic groups for males and females relative to the White ethnic group. We used the White ethnic group as the reference category as it has the largest population. We report the hazard ratios for each minority ethnic group relative to the White ethnic group, after adjusting for age (in green) and for the full range of characteristics described earlier (in blue). The hazard ratio is a measure of how much greater or lesser is the rate of death involving COVID-19 for each minority ethnic group relative to the White population. A hazard ratio greater than one indicates a greater rate of death involving COVID-19 than the reference group, while a hazard ratio less than one indicates a lower rate of COVID-19 mortality than the reference group.
After adjusting for age, men and women from all ethnic minority groups (except females of Chinese ethnic background) are at greater risk of death involving COVID-19 compared with those of White ethnic background. The rate of death involving COVID-19 is 3.3 times greater for Black males than White males, while the rate for Black females is 2.4 times greater. People of Bangladeshi or Pakistani ethnic background had more than twice the rate of death involving COVID-19 than those of White ethnic background (2.5 times for males and 2.0 times for females). People of Indian, Mixed and Other ethnic backgrounds also had statistically significantly raised rates of death involving COVID-19 compared with those of White ethnic background. For the Chinese ethnic group, we find a raised risk among males but not females.
These differences are smaller than those reported in our previous publication, when rates of death involving COVID-19 up until 10 April 2020 were included in the study, suggesting that the increase in mortality risk for ethnic minority groups compared with people of White ethnic background was greater in the early phase of the coronavirus pandemic.
In blue, we show estimates of differences in the risk of death after further adjusting for region, population density, area deprivation, household composition, socio-economic position, household composition and living arrangements with regard to multigenerational households, and measures of occupational exposure to the disease (including key worker status and exposure to others) in 2011. These adjusted results show relative differences in risk between ethnic minority groups and the White population that are not explained by the factors included in the model. More information on how the hazard ratios change when adjusting for different sets of characteristics can be found in the technical appendix in addition to model diagnostics.
Adjusting for these factors substantially reduces the estimated risk of death involving COVID-19 for ethnic minority groups relative to the White population. After adjusting for these factors, the rate of death involving COVID-19 among Black males remains twice as great as that for comparable White males. Rates of COVID-19 mortality experienced by males of Bangladeshi or Pakistani and Indian ethnic background are 1.5 and 1.6 times greater than those for similar White males. After adjusting for these characteristics, males of Chinese and Mixed ethnic backgrounds are not at significantly greater risk than White males.
Comparing the age-adjusted and fully adjusted hazard ratios suggests that these factors explain a substantial part of the raised rate of death experienced by ethnic groups compared with the White ethnic group. Among males, these factors explain about two-thirds of the raised risk for Bangladeshi or Pakistani ethnic background, more than half for Black and about 40% for Indian ethnic backgrounds respectively.
Adjusting for these factors reduces the size of the hazard ratios between ethnic minority groups and the White ethnic group to a greater extent for females. Once we adjust for these factors, females from Bangladeshi or Pakistani and Mixed ethnic backgrounds are not at significantly greater risk than White females. These factors explain about 70% of the raised risk for Black females and 80% for Indian females. After adjusting for these factors, the rate of death involving COVID-19 for Black females remains 1.4 times greater than that for White females, while the rate for Indian females is 1.1 times greater.
To gain a better understanding of the differences in risk of death involving COVID-19 across ethnic groups, we investigate whether these differences are more marked in some demographic and socio-economic groups than others. To do so, we estimate Cox proportional hazard models separately for different population segments. First, we examine whether the differences in deaths involving COVID-19 vary across age groups by estimating separate models for people aged under 70 years and people aged 70 years or over. We find that differences across ethnic groups alter across age groups. The differences in mortality risk are larger for younger (people aged under 70 years) than older people, as shown in Section 4: Age-standardised mortality rates of death involving COVID-19 by ethnic group. The pattern is similar for males and females. This could be partly explained by the greater likelihood of this population being economically active and in employment; although we account for some measures of occupational exposure, an imbalance across ethnic groups in likelihood to be working in at-risk occupations, such as front-facing occupations, could be a determining factor yet to be explored in detail with additional data sources.
We also investigated whether differences in deaths involving COVID-19 across ethnic groups vary by measures of deprivation and socio-economic status. In the census, the National Statistics Socio-economic Classification (NS-SEC) is not consistently available for individuals aged 75 years or over; therefore, we could not use this variable to stratify the analysis. Instead, we focused on household deprivation2 and the level of the highest qualification (degree or not) obtained from the 2011 Census. We find that differences in the risk of death between ethnic minority groups and the White population tend to be larger among non-deprived households and those with a degree.
We also examined whether differences across ethnic groups vary depending on whether individuals were key workers. To do this, we used occupational status from the 2011 Census as a proxy for current occupation. We restricted our sample to those of working age in March 2020 and estimated the models separately for those who in 2011 were in an occupation listed as key workers and those who were not in 2011. We found that the differences across ethnic groups were more pronounced among those who were not key workers.
Overall, we have found evidence that the ethnic differences are more pronounced among the groups that are at lower risk of dying of COVID-19.
Our adjustment for aspects of demographic and socio-economic circumstances is limited since the characteristics we use were retrieved from the 2011 Census. Therefore, these may not accurately reflect the study population’s circumstances in 2020. While we adjust for some dimensions of health, the information collected in 2011 is limited and does not distinguish between different types of co-morbidities, which are a likely modifier of these differential risks observed. Some ethnic groups may have a greater propensity to suffer from co-morbidities that are associated with worse outcomes among those infected by COVID-19, which we plan to take account of in future analyses. A study based on electronic health records found that even after adjusting for co-morbidities, ethnic minority groups were still at greater risk of death involving COVID-19. However, their set of demographic and socio-economic characteristics were limited. Combining the wide range of socio-economic characteristics from the census to data on co-morbidity may provide better evidence on differences in deaths involving COVID-19 across ethnic groups.
Notes for: Ethnic group differences in deaths involving COVID-19, adjusted for socio-demographic factors
In the previous publication we used logistic regression to model the probability of death involving COVID-19. In theory, the Cox proportional hazards model is more appropriate to model the risk of death from a given cause as it accounts not only for whether the individual dies from this disease occurs but also the timing of the death, and death from other causes. Because the period at risk is short, we obtain very similar results when using logistic regression models instead.
The dimensions of deprivation used to classify households are indicators based on four selected household characteristics – education, employment, health and housing. Thus, households can be deprived in up to four dimensions.
6. Glossary
Age-standardised mortality rates
Age-standardised mortality rates (ASMRs) are used to allow comparisons between populations that may contain different proportions of people of different ages. The 2013 European Standard Population is used to standardise rates.
Cox proportional hazards regression model
The Cox proportional hazards regression model is a multiple regression procedure that measures the association between a time-to-event outcome and a characteristic of interest such as disability, while adjusting for other characteristics expected to also be associated with the outcome.
Hazard ratio
A hazard ratio is a measure of the relative differences in the instantaneous rate of mortality between groups. A hazard ratio greater than one indicates the rate of mortality is higher, and likewise less than one lower, in the population group under study compared with a reference group.
Coronaviruses
The World Health Organization (WHO) defines coronaviruses as “a large family of viruses that are known to cause illness ranging from the common cold to more severe diseases such as Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS)”. Between 2001 and 2018, there were 12 deaths in England and Wales due to a coronavirus infection, with a further 13 deaths mentioning the virus as a contributory factor on the death certificate.
Coronavirus (COVID-19)
COVID-19 refers to the “coronavirus disease 2019” and is a disease that can affect the lungs and airways. It is caused by a type of coronavirus. Further information is available from the WHO.
Back to table of contents