Table of contents
- Background and definition
- What are legal highs?
- Blanket ban on psychoactive substances
- Deaths involving legal highs, heroin and cocaine
- Trends in legal high deaths over time
- Deaths involving legal highs: by sex
- Deaths involving legal highs: by age
- Legal high deaths involving other drugs or alcohol
- Impact of banning mephedrone
- So why are legal highs dangerous?
- Methodological considerations
- References
- Background notes
1. Background and definition
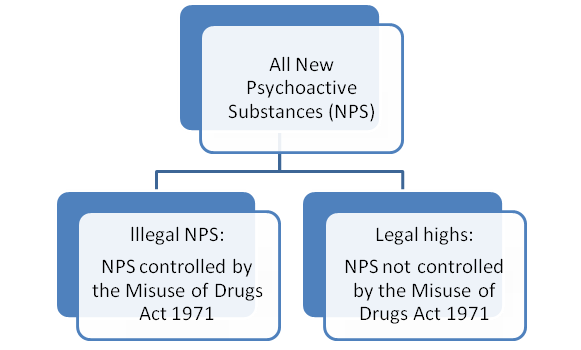
New psychoactive substances (NPS) started to become more popular on the UK drugs scene around 2008 to 2009, with synthetic stimulants such as benzylpiperazine (BZP) and mephedrone, and synthetic cannabinoids (such as "Spice"), among the first to gain popularity. NPS are sometimes referred to as legal highs, but many are now controlled under the Misuse of Drugs Act 1971, so are no longer legal.
Diagram 1: Relationship between legal highs and all new psychoactive substances
Download this image Diagram 1: Relationship between legal highs and all new psychoactive substances
.png (16.6 kB){kind=link}
This article focuses on substances that were not controlled under the Misuse of Drugs Act 1971 on the day the person died, and are referred to as legal highs throughout this article. It covers a 10-year time period from 2004 to 2013. Various drugs on our list have been controlled during this period, consequently, the drugs included in our definition of a legal high change throughout the analysis period, as drugs are removed from the list once they become illegal. For example, mephedrone was banned on 16 April 2010, so deaths involving mephedrone are only included if they occurred between 1 January 2004 and 15 April 2010.
We publish an annual statistical bulletin on Deaths related to drug poisoning in England and Wales, which contains statistics on deaths involving a wide range of substances. Figures on NPS deaths in that bulletin are based on a much broader definition and include drugs that are now controlled under the Misuse of Drugs Act 1971.
Back to table of contents2. What are legal highs?
Legal highs contain substances which produce similar psychoactive effects to "traditional" illegal drugs like cocaine, cannabis and ecstasy. There is no officially agreed list of substances that are categorised as legal highs, but this article concentrates on the following types of substances:
- stimulants like piperazines (for example, BZP), cathinones (for example, mephedrone), benzofurans and methiopropamine
- sedatives such as benzodiazepine analogues (for example, etizolam) and new synthetic opioids
- hallucinogenic drugs like NBOMes and alpha-methyltryptamine
- dissociatives, such as methoxetamine
- synthetic cannabinoids like 5F-AKB-48
We have not included drugs that are sometimes thought of as legal highs, but have actually been used recreationally for many years, such as GHB/GBL. We have also excluded medicines that are licensed for use in the UK, but which are also used recreationally, such as nitrous oxide. A full list of the substances included is available in the Background notes section.
The majority of legal highs are obtained from someone known to the individual (for example, a friend, family, or acquaintance), or from a "headshop", but some are also bought from drug dealers or from the web (Home Office, 2015a). They are generally labelled as being "not for human consumption", and are often marketed as plant food, bath salts, incense or research chemicals. Legal highs are commonly sold under brand names like "Spice", "Clockwork Orange", and "Ivory wave".
Back to table of contents3. Blanket ban on psychoactive substances
The government has already banned a large number of NPS under the Misuse of Drugs Act 1971. However, it has been difficult to control the use of NPS with existing legislation, as when one drug (or group of drugs) is controlled, scientists simply tweak the chemical structure of the drug so that it evades the law. The government, therefore, remains concerned about how quickly NPS are being created and the potential harm they pose. To address this problem they have introduced the Psychoactive Substances Act, which will come into force in spring 2016. This establishes a blanket ban on the importation, production or supply of psychoactive substances, though things like alcohol, tobacco, caffeine and medicines used in healthcare-related activities will be exempt.
Evidence on the harms of a range of NPS are documented in reports by the Advisory Council on the Misuse of Drugs (ACMD), but how many deaths do they actually cause?
Back to table of contents4. Deaths involving legal highs, heroin and cocaine
Figure 1: Number of deaths involving selected substances occurring between 2004 and 2013
England and Wales
Source: Office for National Statistics
Notes:
- Cause of death was defined using the International Classification of Diseases, Tenth Revision (ICD-10) codes shown in the Background notes. Deaths were included where the underlying cause was drug-related and the specified substance was mentioned on the death certificate. If more than one substance was mentioned, the death will be included more than once.
- Figures include deaths of non-residents who died in England or Wales.
- Figures are for deaths occurring, rather than deaths registered in each calendar year. ONS is not usually notified of a death until it has been registered, and due to the length of time it takes to complete a coroner’s inquest, it can take months or even years for a drug-related death to be registered. These figures only include deaths that occurred between 2004 and 2013, and were registered by 31 December 2014. Therefore figures for deaths in 2013 presented here will be an underestimate.
- There is no officially agreed list showing which substances are classed as legal highs, but the full list of substances included in this category within this article can be found in the Background notes.
Download this chart Figure 1: Number of deaths involving selected substances occurring between 2004 and 2013
Image .csv .xlsNumber of deaths involving legal highs is very small compared with heroin/morphine and cocaine
Between 2004 and 2013, there were 76 deaths involving legal highs in England and Wales. Specifically, these are drug-related deaths where the death certificate mentioned a legal high. The death certificate may also mention other drugs or alcohol, so the legal high may not have been the primary cause of death in all of these 76 cases.
To put this in context – over the same 10 year period there were more than 100 times as many deaths involving heroin or morphine (7,748) and more than 20 times as many deaths involving cocaine (1,752) than legal highs.
Back to table of contents5. Trends in legal high deaths over time
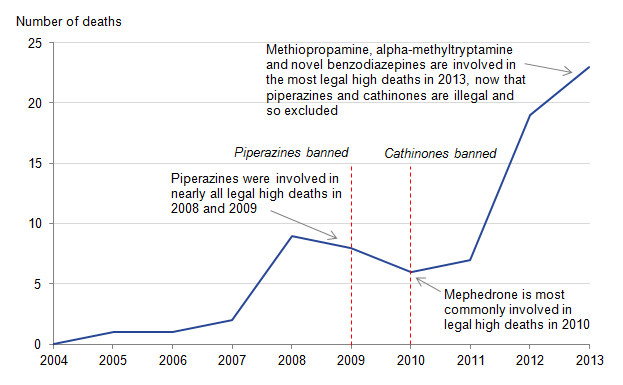
Figure 2: Number of deaths involving legal highs occurring between 2004 and 2013
England and Wales
Source: Office for National Statistics
Notes:
- Cause of death was defined using the International Classification of Diseases, Tenth Revision (ICD-10) codes shown in the Background notes. Deaths were included where the underlying cause was drug-related and a legal high was mentioned on the death certificate.
- Figures include deaths of non-residents who died in England or Wales.
- Figures are for deaths occurring, rather than deaths registered in each calendar year. ONS is not usually notified of a death until it has been registered, and due to the length of time it takes to complete a coroner’s inquest, it can take months or even years for a drug-related death to be registered. These figures only include deaths that occurred between 2004 and 2013, and were registered by 31 December 2014. Therefore figures for deaths in 2013 presented here will be an underestimate.
- There is no officially agreed list showing which substances are classed as legal highs, but the full list of substances included in this category within this article can be found in the Background notes.
Download this image Figure 2: Number of deaths involving legal highs occurring between 2004 and 2013
.png (17.3 kB) .xls (73.7 kB)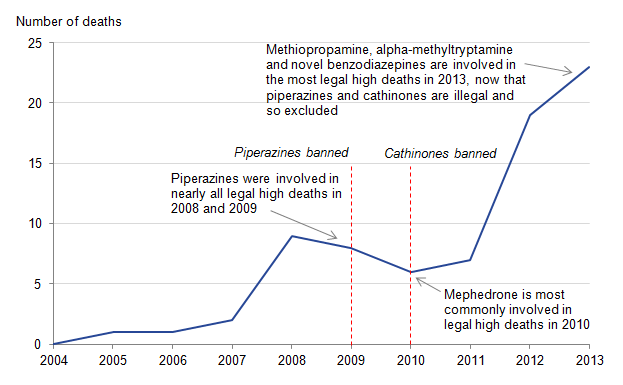{kind=link}
Deaths involving legal highs increase in recent years
Although the number of deaths involving legal highs is small, they have increased over the last decade, from no deaths in 2004 to an estimated 23 deaths in 2013. There has been a marked rise between 2011 and 2013, when deaths have more than tripled from 7 to 23. However, caution needs to be used when interpreting these trends as they are based on very small numbers.
Despite the relatively small numbers, deaths involving legal highs (like all drug-related deaths), are preventable and each one is a tragedy.
Back to table of contents6. Deaths involving legal highs: by sex
Figure 3: Number of drug-related deaths involving legal highs, by sex, deaths occurring 2004 to 2013
England and Wales
Source: Office for National Statistics
Notes:
Cause of death was defined using the International Classification of Diseases, Tenth Revision (ICD-10) codes shown in the Background notes. Deaths were included where the underlying cause was drug-related and a legal high was mentioned on the death certificate.
Figures include deaths of non-residents who died in England or Wales.
Figures are for deaths occurring, rather than deaths registered in each calendar year. ONS is not usually notified of a death until it has been registered, and due to the length of time it takes to complete a coroner’s inquest, it can take months or even years for a drug-related death to be registered. These figures only include deaths that occurred between 2004 and 2013, and were registered by 31 December 2014. Therefore figures for deaths in 2013 presented here will be an underestimate.
There is no officially agreed list showing which substances are classed as legal highs, but the full list of substances included in this category within this article can be found in the Background notes.
Download this chart Figure 3: Number of drug-related deaths involving legal highs, by sex, deaths occurring 2004 to 2013
Image .csv .xlsDeaths involving legal highs increased in males in the last 3 years, but remain stable in females
The majority of deaths involving legal highs are males (5 out of 6 deaths). This is slightly higher than the male to female ratio seen for drug misuse deaths, where about three-quarters of the deaths are males. The first female death involving a legal high shown in this time series occurred in 2009 and female deaths have been low and stable since then. In contrast, male deaths showed a small peak in 2008, before falling slightly, but have increased quite sharply since 2010.
Back to table of contents7. Deaths involving legal highs: by age
Figure 4: Age-specific mortality rate for deaths involving legal highs occurring in 2004 to 2013 combined
England and Wales
Source: Office for National Statistics
Notes:
Age-specific mortality rate per 10 million population.
Cause of death was defined using the International Classification of Diseases, Tenth Revision (ICD-10) codes shown in the Background notes. Deaths were included where the underlying cause was drug-related and a legal high was mentioned on the death certificate.
Figures include deaths of non-residents who died in England or Wales.
Figures are for deaths occurring, rather than deaths registered in each calendar year. ONS is not usually notified of a death until it has been registered, and due to the length of time it takes to complete a coroner’s inquest, it can take months or even years for a drug-related death to be registered. These figures only include deaths that occurred between 2004 and 2013, and were registered by 31 December 2014. Therefore figures for deaths in 2013 presented here will be an underestimate.
There is no officially agreed list showing which substances are classed as legal highs, but the full list of substances included in this category within this article can be found in the Background notes.
Download this chart Figure 4: Age-specific mortality rate for deaths involving legal highs occurring in 2004 to 2013 combined
Image .csv .xlsMost legal high deaths happen in people aged 20 to 29
The average (median) age for deaths involving a legal high is 28, which is younger than for drug misuse deaths, where the average age is 38. The youngest person to die after taking a legal high was aged 18 and 9 teenagers have died from this between 2004 and 2013. In fact, the highest mortality rate is in people aged 20 to 29, at just over 4 deaths per 10 million population. Deaths involving legal highs then decline with age.
Back to table of contents8. Legal high deaths involving other drugs or alcohol
One of the difficulties with interpreting drug-related mortality data is that the deaths often involve more than one substance and it is impossible to tell from the death certificate which substance was primarily responsible for the death.
Figure 5: Percentage of legal high deaths that also involve alcohol or another drug, occurring in 2004 to 2013 combined
England and Wales
Source: Office for National Statistics
Notes:
Cause of death was defined using the International Classification of Diseases, Tenth Revision (ICD-10) codes shown in the Background notes. Deaths were included where the underlying cause was drug-related and the specified substance was mentioned on the death certificate. If more than one substance was mentioned, the death will be included more than once.
Figures include deaths of non-residents who died in England or Wales.
Figures are for deaths occurring, rather than deaths registered in each calendar year. ONS is not usually notified of a death until it has been registered, and due to the length of time it takes to complete a coroner’s inquest, it can take months or even years for a drug-related death to be registered. These figures only include deaths that occurred between 2004 and 2013, and were registered by 31 December 2014. Therefore figures for deaths in 2013 presented here will be an underestimate.
There is no officially agreed list showing which substances are classed as legal highs, but the full list of substances included in this category within this article can be found in the Background notes.
Single legal high deaths are those where only one substance was mentioned on the death certificate, that is, no alcohol or any other drug was mentioned.
Figures may not add to 100, due to rounding.
Download this chart Figure 5: Percentage of legal high deaths that also involve alcohol or another drug, occurring in 2004 to 2013 combined
Image .csv .xlsAround 60% of legal high deaths also involve another drug or alcohol
Between 2004 and 2013, alcohol was involved in about 10% of legal high deaths, though none of the 23 deaths in 2013 mentioned it. So alcohol is involved in proportionally fewer legal high deaths compared with drug misuse deaths, where about 1 in 3 also involve alcohol.
Over the same period, 57% of deaths involving legal highs mentioned more than one drug, but in 2013 this proportion dropped to about a third. These deaths could involve a combination of legal highs and illegal drugs or a mixture of different legal highs and the deaths may or may not have also involved alcohol. For drug misuse deaths the proportion involving more than one drug was much lower – 35% between 2004 and 2013; but this proportion has been gradually increasing over time. Forensic testing of NPS has shown that a single tablet or powder can contain a mixture of different NPS and even "traditional" illegal drugs (Home Office, 2015b). This may partly explain the high proportion of legal high deaths which involve multiple drugs, as users may not even be aware that they are taking more than one substance.
As the number of deaths involving legal highs is very small, it is hard to identify clear patterns of drug combinations. Nevertheless, there is an indication that deaths in 2008 and 2009 often involved a combination of piperazines and ecstasy or cocaine. However, the combinations of drugs that lead to death may not be representative of the pattern of drug taking in the population.
More recently, the deaths data suggests a trend for taking several new psychoactive substances together, some of which may have been recently banned – for example, taking methiopropamine and a cathinone. Deaths also happen when legal highs are taken with more traditional stimulants such as amphetamines. An emerging trend in the deaths data is the combination of an opioid drug like heroin/morphine, methadone or tramadol with a novel benzodiazepine such as phenazepam or etizolam. This mirrors the established pattern of taking an opioid drug with a traditional benzodiazepine like diazepam.
Back to table of contents9. Impact of banning mephedrone
The previous sections looked at deaths where the substances involved were legal at the time of death. This section contains a case study of mephedrone – one of the first legal highs to catch the media’s attention – and looks at trends in deaths before and after it was banned. Mephedrone, sometimes called "Meow meow" or "M-Cat" is a cathinone which was controlled as a Class B substance under the Misuse of Drugs Act 1971 on 16 April 2010, along with a number of other cathinones.
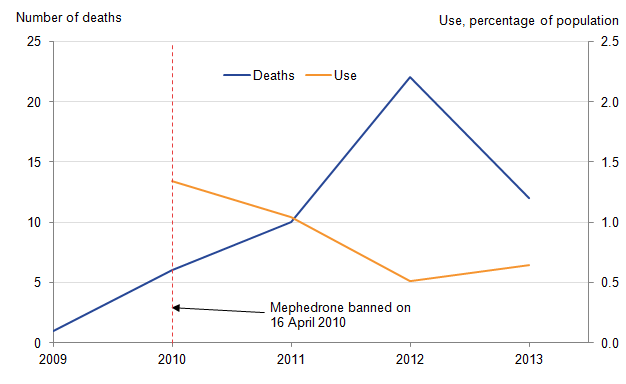
Figure 6: Number of deaths involving mephedrone and proportion of people reporting mephedrone use in the previous year, 2009 to 2013
England and Wales
Source: Office for National Statistics & Home Office
Notes:
- Cause of death was defined using the International Classification of Diseases, Tenth Revision (ICD-10) codes shown in the Background notes. Deaths were included where the underlying cause was drug-related and mephedrone was mentioned on the death certificate.
- Figures for mephedrone use were taken from the Home Office's Crime Survey for England and Wales (CSEW) and are collated based on financial years. Figures for deaths were collated based on the calendar year the death occurred. For example, figures for 2010 show mephedrone use in the previous 12 months reported in the 2010/11 CSEW; and deaths occurring between January and December 2010.
- ONS is not usually notified of a death until it has been registered, and due to the length of time it takes to complete a coroner’s inquest, it can take months or even years for a drug-related death to be registered. These figures only include deaths that occurred between 2009 and 2013, and were registered by 31 December 2014. Therefore figures for deaths in 2013 will be an underestimate.
- Figures for mephedrone use are for people aged 16 to 59 only. All deaths involving mephedrone were people in this age range, so figures on deaths and use are broadly comparable.
- Use of Mephedrone in the last year was included for the first time in the CSEW, 2010/11, so figures are not available for 2009.
Figures include deaths of non-residents who died in England or Wales.
Download this image Figure 6: Number of deaths involving mephedrone and proportion of people reporting mephedrone use in the previous year, 2009 to 2013
.png (12.9 kB) .xls (58.9 kB)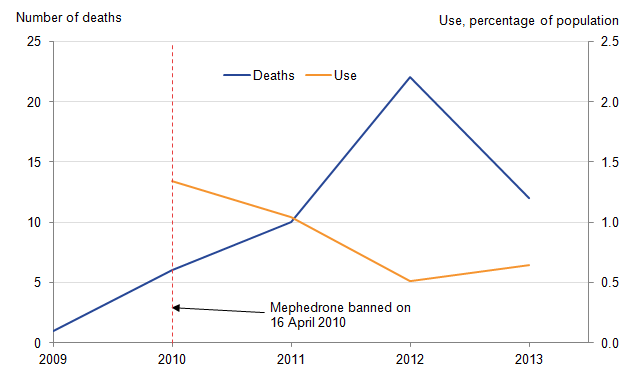{kind=link}
Deaths involving mephedrone did not immediately fall after it was banned
The first death involving mephedrone occurred in 2009, and deaths continued to rise for several years following the ban, peaking at 22 deaths in 2012, before falling to 12 deaths in 2013. This suggests that banning mephedrone did not immediately reduce the number of mephedrone-related deaths. However, it is possible that mephedrone use would have increased and deaths would have been even higher, had it not been banned.
Mephedrone was first included in the Crime Survey for England and Wales – CSEW – (Home Office, 2015a) in 2010/11, when 1.3% of 16 to 59-year-olds reported using mephedrone in the last year, although the figure was higher for young people – 4.4% of 16 to 24-year-olds. Use had dropped to 0.6% of 16 to 59-year-olds in the 2013/14 CSEW (around 211,000 people) and to 1.9% of 16 to 24-year-olds.
The trend in use of mephedrone is not consistent with the number of deaths, which peaked in 2012, but by then the proportion of people using mephedrone had more than halved. At first glance, this pattern might suggest that people were less willing to admit to taking mephedrone since it was banned. However, the majority of people who reported using mephedrone in the Crime Survey, also reported using another illegal drug, so it’s not clear whether banning mephedrone would suddenly lead to under-reporting of its use.
There is unlikely to be a simple explanation of why deaths involving mephedrone continued to increase while use apparently declined. It may be that the drugs that people are now taking with mephedrone are more dangerous; or they are using riskier methods to take mephedrone (for example, injecting instead of snorting); it could be that people are experiencing increasing harm having used mephedrone for a longer period of time, with escalating doses leading to more fatal overdoses; or it is possible that a more vulnerable group of people have begun using mephedrone. In addition, it is possible that people stockpiled mephedrone before it was banned, which may have affected patterns of use after the ban. Any of these factors could have lead to the increases in deaths involving mephedrone seen between 2009 and 2012. The fact that deaths involving legal highs in general continued to rise in 2013, while deaths involving mephedrone fell, may suggest mephedrone is becoming less popular and people are now taking different types of NPS.
These data suggest there is a complex relationship between a drug’s legal status, how widely it is used in the population and the number of deaths that occur. And it will be interesting to see what impact the introduction of the Psychoactive Substances Act 2016 will have on the longer term trends in deaths involving NPS.
Back to table of contents10. So why are legal highs dangerous?
Some people think that because these drugs are (or were recently) legal, they are safe, but this isn’t the case. The potential short-term effects of legal highs include agitation, paranoia, psychosis, delirium, tachycardia, hypertension, chest pain, seizures and elevated temperature; and overdoses of legal highs may require emergency hospital treatment. In addition to immediate health effects, use of legal highs can impact on people’s employment and education (ACMD, 2011). More information on the harms associated with use of legal highs can be found in ACMD risk assessments.
Importantly, users cannot be sure what substance they are actually taking, how much to take, what effect it will have or whether it is still legal. In addition, there has been very little research into the long-term harms, so users act as "human guinea pigs".
As the majority of legal highs have only been used for a few years at most, we don’t know how harmful these drugs could be if a person became dependent and used them in high doses, repeatedly, over a long period of time. It is possible that in these circumstances they may cause significant long-term mental or physical health problems. Moreover, we don’t know whether under the right social conditions an increasing number of people could become dependent on any of these drugs, possibly one of the synthetic opioids like AH-7921, resulting in much greater harm.
So although deaths involving legal highs are small compared with "traditional" drugs, taking them is still very risky.
Back to table of contents11. Methodological considerations
Registration delays
Due to the length of time it takes to complete a coroner’s inquest there can be a considerable delay between when a death occurred and when it was registered (5 to 6 months on average for drug-related deaths). All data presented above are based on the date the death occurred, not when it was registered. Due to registration delays, many of the deaths that occurred in 2014 and some of those that occurred in 2013 will not have been registered when this data extract was taken (that is, by 31 December 2014). Therefore figures for 2014 are not presented as they are too incomplete and figures for 2013 should also be treated with caution, as they are likely to be an underestimate of the total number of legal high deaths occurring in that year.
Data on drug-related deaths registered in 2015 are currently being processed and figures will be published on our website in September 2016.
Other limitations of ONS drug-related deaths data
The figures on deaths involving legal highs reported in this article are likely to be an underestimate of the true numbers and need to be interpreted with caution for the following reasons:
- the number of deaths is very small, making it harder to interpret changes from one year to the next
- these figures are based only on information reported on the coroner’s death certificate so may not include every substance involved in the death
- there may not be toxicology tests available to detect the newest psychoactive substances, and coroners may not be able to afford to test for every new substance: this is especially the case in deaths where a more common substance such as heroin or cocaine has already been found at post-mortem
- alternatively, the increases in legal high deaths in recent years may be due to coroners becoming more aware of these substances and so they are more likely to be tested for at post-mortem
- in around 1 in 10 drug poisoning deaths, only a general description is recorded on the coroner’s death certificate (such as drug overdose or multiple drug toxicity)
- in around 30% of all drug poisoning deaths, the death certificate mentions more than one specific drug; where more than one drug is mentioned, it is not possible to tell which was primarily responsible
- approximately 30% of all drug-related poisoning deaths also contain a mention of alcohol or a consequence of long-term alcohol abuse (for example, cirrhosis) in addition to a drug
12. References
Advisory Council on the Misuse of Drugs – ACMD (2011) ‘Consideration of the Novel Psychoactive Substances (‘Legal Highs’)’, accessed on 21 April 2016.
Advisory Council on the Misuse of Drugs – ACMD (2016) Risk assessments of a range of NPS, accessed on 21 April 2016.
Home Office (2015a) Crime Survey for England and Wales 2014/15, accessed on 21 April 2016.
Home Office (2015b), Annual Report on the Home Office Forensic Early Warning System (FEWS), accessed on 21 April 2016.
The Misuse of Drugs Act (1971), accessed on 21 April 2016.
Office for National Statistics (2014), ‘Deaths related to drug poisoning in England and Wales’, accessed on 21 April 2016.