Table of contents
- Introduction
- Collaboration
- Relevance to policy
- Overview of methodological aspects
- What is the impact of changes in aspects of the methodology on survival estimates?
- Why does the change in age-weighting systems result in these differences in the survival estimates?
- Overall conclusion of impact
- Which publications will be impacted?
- References
- Appendix 1: Weighting
- Appendix 2: Adult survival comparisons
- Appendix 3: Definition of cancers
- Appendix 4: Interpretation of a box plot
1. Introduction
From February 2018, the Office for National Statistics (ONS) and Public Health England (PHE) partnership will publish sub-national cancer survival estimates in the Geographic patterns of cancer survival in England National Statistics bulletin. This follows on from working in partnership to collaboratively produce the national (England) cancer survival estimates published in June 2017 and the Index of cancer survival for Clinical Commissioning Groups in England published in November 2017.
This report compares the methods that will be applied from February 2018 in producing these sub-national survival statistics to methods used previously. The approach improves comparability with international cancer statistics and is consistent with the methodology applied to the national cancer survival estimates since June 2017.
Correction, 13th April 2018
Following publication on Monday 19th February 2018, a correction to the 2007 to 2011 dataset published alongside this methodology paper was identified. This was due to a small error in the patient population affecting both the patient counts and cancer survival estimates. We have re-published and corrected this error in Tables 1, 2, 5, 8, 10 and 11 (labelled Tables 1 to 6 in the previous version of this data) in the dataset. You can see the original version of this data on the previous versions page.
Table 3, Figure 3 and some accompanying text have also been updated in Section 5 to reflect these changes. We apologise for any inconvenience.
Back to table of contents2. Collaboration
This publication is produced in partnership with Public Health England Cancer Survival Team, part of the National Cancer Registration and Analysis Service (NCRAS).

3. Relevance to policy
The official statistics on cancer survival form an evidence base to inform cancer policy and programmes that aim to improve cancer outcomes. The statistics are commissioned by the Department of Health and are used to:
help inform government policy on cancer
provide non-government bodies with accurate and timely data on the disease
provide citizens with accessible data on the disease to help inform debate
To ensure the data are relevant, the Office for National Statistics (ONS) and Public Health England (PHE) strive to produce estimates that are timely, accurate and accessible.
Given that a significant gap remains in survival compared with the European average, the Department of Health identified cancer as a specific improvement area for preventing people dying prematurely in the National Strategy (announced in 2011). In 2015, a new five year cancer strategy for England (PDF, 4.90MB) was developed by the Independent Cancer Taskforce, which sets out recommendations for how the NHS can improve cancer outcomes for patients. The new strategy is being reviewed by government bodies.
Cancer survival estimates also feed into outcomes strategies that set out how the NHS, public health and social care services will contribute to the progress agreed with the Secretary of State, in each of the high-level outcomes frameworks. The indicators set for the National Health Service (NHS) Outcomes Framework include 1-year and 5-year survival for all cancers combined and separately for colorectal, breast and lung cancer at Clinical Commissioning Group (CCG) level. Specifically, these sub-national cancer survival estimates feed into the Compendium of Population Health Indicators, which is useful for comparing the health profiles of local areas.
Back to table of contents4. Overview of methodological aspects
The following elements of cancer survival methodology are compared in Table 1:
the cancer registrations that are included in the analysis (exclusion and inclusion criteria)
the type of survival estimator
the weights used to age-standardise the estimates
the version of International Coding Definition (ICD) used to define cancer sites
the tumour sites included in the bulletin
the non-standardised survival estimates used in the accompanying trend analysis
Table 1: Summary of methods used in the Geographic patterns of cancer survival statistical bulletin
Method |
Rationale |
Outcome |
|---|---|---|
Exclusion and inclusion criteria |
We will continue to use the same criteria that have been historically applied. The method is outlined in the Control of data quality for population – based cancer survival analysis paper (Li R 2014). These are supplemented by further data quality checks proposed by the European Network of Cancer Registrations (ENCR) (Martos C 2014). |
No change in method. |
Survival estimation method |
Since 2012, net survival (Pohar Perme M 2012), using an unbiased estimator, has been used instead of relative survival. The partnership will continue to produce net survival estimates, in line with the national (England) statistics in cancer survival. This is the most appropriate method for official statistics as it: - removes the effect of general mortality, so only reflects “excess” mortality due to diagnosis of cancer - is internationally comparable, with a growing will within the UK and Ireland Association of Cancer Registries to move to the same methods and eventually UK-wide statistics However, to make the geographic patterns of cancer survival more comparable with the national method, we will make two changes: - move to using the complete approach, rather than the cohort - move to using five years of aggregated data, rather than three years of aggregated data |
We will continue to produce net survival estimates for one year and five years of follow-up. We will be moving to use the complete approach on five years of aggregated data for age-standardised survival estimates. We will continue to produce single year un-standardised survival estimates. |
Weights used to age-standardise the estimates |
The weights historically used for age standardisation were based on the proportions of cancer diagnoses in England and Wales from 1996 to 1999 in each age group, sex and type of cancer. |
We will be moving to the International cancer patient population for age standardising survival ratios (ICSS) (Corazziari I 2004) for the publications from February 2018 onwards. |
ICD coding version |
Currently, the tumour sites in all joint ONS and PHE cancer survival, incidence and mortality bulletins are defined using the International Classification of Diseases 10th Revision (ICD10-O2) (Table A5, Appendix 3). Clinical practice and evidence now suggests that a move to ICD-O-3 would produce more homogenous cohorts. |
No change in method at present. Being considered for future publications. |
Tumour sites included in the bulletin |
Previous bulletins include the following cancer sites: - Oesophagus (C15) - Stomach (C16) - Colon (C18) - Lung (C33 to C34) - Breast (in women, C50) - Cervix (in women, C53) - Prostate (in men, C61) - Bladder (C67) |
We will additionally include the following cancer sites: - Colorectum (C18 to C20 and C21.8) - Kidney (C64 to C66 and C68) - Myeloma (C90) - Non-Hodgkin lymphoma (C82 to C85) - Rectum (C19 to C20 and C21.8) - Uterus (in women, C54 to C55) By using five years of aggregated data, it will now be possible to produce robust age-standardised estimates for a more representative selection of cancer sites at sub-national levels. |
Non-standardised survival estimates used in trend analysis |
We will continue to use single year non-standardised estimates to assess the annual change in net survival. However, they are under review as using age-standardised and aggregated estimates for the trend analysis would be more consistent with the published estimates. |
No change in method at present but, for reasons of follow-up, the years to assess trend in 1-year and 5-year survival estimates will differ. Considering moving to use three or five years of aggregated data in the time series of future publications. Using aggregated data will potentially allow for age-standardised results to be compared over time. |
In summary, the main changes to the method for the upcoming Geographic patterns of cancer survival statistical bulletin are:
the adoption of the International Classification of Survival Standard (ICSS) international cancer patient population for age standardising survival ratios
using the complete approach on five years of aggregated data for age-standardised survival estimates
- expanding the analysis to include a wider range of cancer sites
The reasons for adopting the ICSS patient population are:
the ICSS weights are publicly and readily available
these weights are widely used, for example, in the UK by Northern Ireland and Scotland and internationally by the United States National Cancer Institute and by the International Cancer Benchmark Partnership
the ICSS weights continue to vary by tumour type reflecting age distributions of the different cancers
to bring the geographic patterns of cancer survival methods in line with the national methodology, by including sub-national estimates for additional cancer sites and by providing more up-to-date estimates for patients diagnosed most recently by moving to the complete approach
it will enable sub-national and national comparisons within England and be a step forward towards national comparisons within the UK and international comparisons of survival estimates
Summary of the International Cancer Survival Standard for age-standardisation
When studying diseases in a population, many of these diseases and their effects are closely related to age. Although comparing survival rates for specific age-groups can be informative, it is often useful to be able to have a summary of survival for every patient in the population diagnosed with a type of cancer. Comparisons using a summary estimate made over time or between geographies can be misleading if the age profiles of the underlying populations are different.
To overcome these potential drawbacks, a weighted average of the age-specific rates is calculated; this process is called age-standardisation. The weights used are independent of geography and time, so they allow for direct comparison of survival estimates over time and between different geographically-defined populations.
Many types of cancer, like lung cancer, are more commonly diagnosed as age increases; others, like Hodgkin’s lymphoma, are more commonly found in younger people. There are also cancers, like brain cancer, that have two peaks in the age distribution where they are commonly diagnosed in the younger and older age-groups but are less commonly diagnosed in middle age. A fourth profile, similar to the first group, is observed for prostate cancer but is far less likely to occur in younger men than other cancers fitting the first profile.
The ICSS system of weights (Table A2) results from analysing which cancer types best fit one of the population profiles described above. An optimal set of weights is then determined that provides the largest number of estimates with good agreement between the standardised and raw survival estimates. There are four sets of weights, reflecting the four commonly observed age profiles of diagnosing different cancers and the weights are set out in Table A2.
Summary of the change from cohort to complete approach
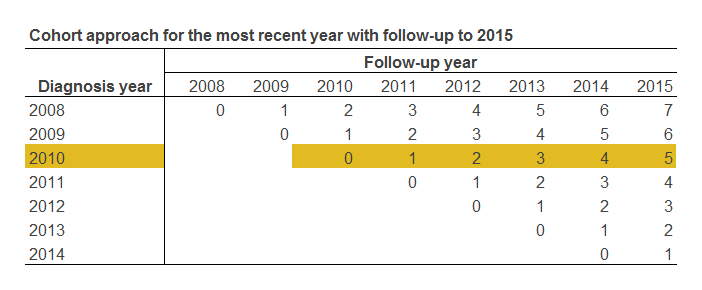
The complete approach allows more reliable estimates than the cohort approach, particularly for smaller geographic regions and less prevalent cancer sites, over the same time period. This is because the complete approach uses all patients diagnosed from a particular year onwards up to the most recent year with follow-up. For example, 5-year survival from 2007 using the cohort approach only uses patients diagnosed in 2007. Whereas, the complete approach would include patients diagnosed between 2007 and 2011.
The survival approach diagrams (Figure 1 and Figure 2) highlight the diagnosis year for the demonstrated approach and the patient years of follow-up included in that approach. A patient pathway begins with diagnosis in year 0 when there are no years of follow-up, this continues right across the diagram increasing for each year of follow-up. For example, patients diagnosed in 2008 with follow-up until 2015 have at least seven years of follow-up. These diagrams focus on 5-year survival.
Cohort approach
Figure 1 highlights 5-year survival using the cohort approach. This approach requires at least five complete years of potential follow-up for each patient. It’s the simplest approach as all patients could be diagnosed in the same year and potentially followed up for the same length of time, as shown in Figure 1.
However, it could also be used for patients diagnosed in different years, for example, to calculate survival for patients diagnosed in 2008 to 2010; as long as all patients have full follow-up available for the latest year. The restriction with this approach is that it has implicit latency and cannot be calculated until at least five years have passed.
Figure 1: An overview of the cohort approach for survival analysis, follow-up to 2015
Source: Office for National Statistics
Download this image Figure 1: An overview of the cohort approach for survival analysis, follow-up to 2015
.PNG (9.9 kB){kind=link}
Complete approach
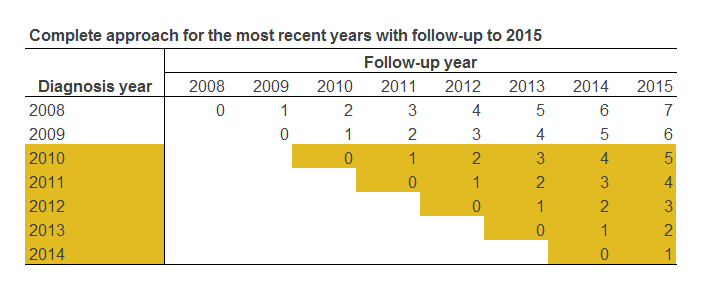
The complete approach to survival analysis, a variant of the classical cohort approach, is used when some patients may have been followed up for less than the full period. For example, it is viable to use the complete approach to produce estimates for patients diagnosed during 2010 to 2014 with follow-up until 31 December 2015, even though not every patient has had the opportunity to be followed up for the full five years. In this example, the potential follow-up time varies between a single year and five years, depending on the year of diagnosis.
Figure 2 highlights the complete approach for 5-year survival. This approach uses all potential years of follow-up for patients diagnosed in a five-year period. The advantage to this approach is it combines timeliness and efficiency using all the available follow-up. However, this approach cannot be used to give an estimate for a single diagnosis year.
Figure 2: An overview of the complete approach for survival analysis, follow-up to 2015
Source: Office for National Statistics
Download this image Figure 2: An overview of the complete approach for survival analysis, follow-up to 2015
.PNG (10.9 kB)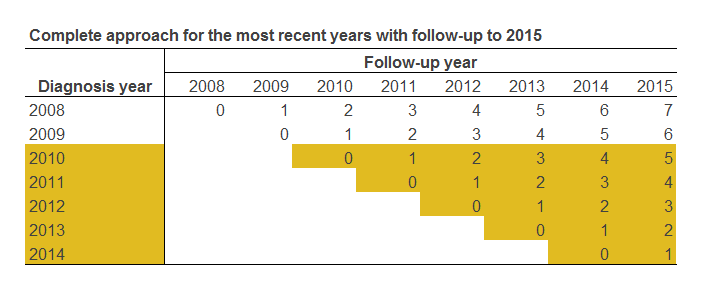{kind=link}
Assessing the impact of methodology changes
This impact paper will be accompanied by the publication of the 2007 to 2011 datasets for the eight cancer sites included in the previous release. Since the previous release covered 2008 to 2010 under the three diagnosis years cohort approach, presenting 2007 to 2011 represents the most consistent match, under the new five diagnosis years approach, as both datasets are centred on 2009. As there is now five complete years of follow-up for these data, both datasets are measured under the cohort approach.
The inclusion of two additional diagnosis years in the age-standardised survival estimates results in the patient counts, presented in the datasets, increasing by approximately two-thirds.
The differences between the two sets of results are due to:
1) the move to the International cancer patient population for age standardising survival ratios (ICSS) weights
2) the aggregation being based on five diagnosis years rather than three
Looking ahead to the Geographic patterns of cancer survival statistical bulletin, the most visible change is in the presented data. The complete approach will enable the publication of 2011 to 2015 data whereas, under the cohort approach, the latest available data would be 2011 due to the requirement for five years of complete follow-up. The statistical bulletin will be accompanied by the publication of analysis for the three interim years (between 2008 to 2012 and 2010 to 2014).
These changes to the methodology will allow the geographic patterns of cancer survival data to be more easily compared with that of the national (England) data. Information about the complete approach to calculating cancer survival can be found in the Cancer survival Quality and Methodology Information report.
There has been no change in methodology used to produce the non-standardised estimates by single year of diagnosis. However, the move from the cohort to the complete approach means that the period covered by the trend analysis will vary for 1-year and 5-year survival.
For both the 1-year and 5-year survival, the trend analysis will be based on the latest available eight non-standardised years (with follow-up), which is consistent with previous releases. However, the complete approach means that for 1-year survival the trend analysis will be based on 2008 to 2015, while the 5-year survival trend will be based on 2004 to 2011. For previous releases, the 1-year and 5-year survival trends were based on the same eight-year period.
Back to table of contents5. What is the impact of changes in aspects of the methodology on survival estimates?
England-level comparison
To assess the impact of the change in the age-standardised weighting, we have run the new method on a comparable cohort of cancer registrations that was used to produce the survival estimates published in 2017 (Difference column, Table 2). The use of estimates centring around 2009 is considered the best proxy for both methods although the estimates produced by the new methodology are based on five years, rather than three years, so contain additional data from patients diagnosed in 2007 and 2011.
Some differences will follow from the extra data included in the estimates. Using three diagnosis years produces estimates that do not pass current data quality tests, so a direct comparison of changing weights between the published estimates and the new methodology is not possible. The age-weights associated with the analysis can be found in Tables A1 and A2 of Appendix 1.
Table 2: Comparison of 1-year and 5-year age-standardised net survival estimates, adults (aged 15 to 99 years) diagnosed from 2007 to 2011 and followed up to 2016, England, for eight common cancer sites
| With the (1) previously published estimates and (2) updated data from Public Health England using complete approach and ICSS weights. | ||||||||
| Net survival estimates | % point difference | |||||||
|---|---|---|---|---|---|---|---|---|
| Site | Sex | Survival length (years) | Published estimates 2008 to 2010 (1) | Updated data with ICSS weights 2007 to 2011 (2) | Difference (2) - (1) | |||
| Bladder | Men | One | 77.8% | 78.5% | 0.7 | |||
| Five | 58.0% | 57.5% | -0.5 | |||||
| Women | One | 67.5% | 66.7% | -0.8 | ||||
| Five | 47.7% | 47.1% | -0.6 | |||||
| Persons | One | 75.1% | 75.2% | 0.1 | ||||
| Five | 55.4% | 54.6% | -0.8 | |||||
| Breast | Women | One | 95.6% | 94.7% | -0.9 | |||
| Five | 84.9% | 82.1% | -2.8 | |||||
| Cervix | Women | One | 82.5% | 79.6% | -2.9 | |||
| Five | 65.5% | 58.0% | -7.5 | |||||
| Prostate | Men | One | 93.1% | 95.1% | 2.0 | |||
| Five | 81.4% | 84.3% | 2.9 | |||||
| Colon | Men | One | 73.5% | 75.3% | 1.8 | |||
| Five | 56.0% | 56.6% | 0.6 | |||||
| Women | One | 73.1% | 74.5% | 1.4 | ||||
| Five | 56.2% | 56.6% | 0.4 | |||||
| Persons | One | 73.2% | 74.9% | 1.7 | ||||
| Five | 56.0% | 56.6% | 0.6 | |||||
| Lung | Men | One | 29.9% | 30.7% | 0.8 | |||
| Five | 9.0% | 9.2% | 0.2 | |||||
| Women | One | 34.4% | 35.2% | 0.8 | ||||
| Five | 11.9% | 12.0% | 0.1 | |||||
| Persons | One | 31.9% | 32.7% | 0.8 | ||||
| Five | 10.3% | 10.5% | 0.2 | |||||
| Oesophagus | Men | One | 41.2% | 42.7% | 1.5 | |||
| Five | 12.8% | 12.6% | -0.2 | |||||
| Women | One | 39.6% | 42.4% | 2.8 | ||||
| Five | 14.9% | 14.6% | -0.3 | |||||
| Persons | One | 40.4% | 42.3% | 1.9 | ||||
| Five | 13.2% | 13.0% | -0.2 | |||||
| Stomach | Men | One | 43.5% | 44.9% | 1.4 | |||
| Five | 17.7% | 18.1% | 0.4 | |||||
| Women | One | 42.8% | 43.4% | 0.6 | ||||
| Five | 19.2% | 19.9% | 0.7 | |||||
| Persons | One | 43.2% | 44.3% | 1.1 | ||||
| Five | 18.2% | 18.6% | 0.4 | |||||
| Source: National Cancer Registration and Analysis Service within Public Health England; Office for National Statistics | ||||||||
Download this table Table 2: Comparison of 1-year and 5-year age-standardised net survival estimates, adults (aged 15 to 99 years) diagnosed from 2007 to 2011 and followed up to 2016, England, for eight common cancer sites
.xls (32.3 kB)Table 2 shows that the impact from changing age-weights combined with expanding the diagnosis data used.
The absolute differences of 1-year survival, in Difference A, range from 0.7% to 2.0% in males (bladder and prostate cancer respectively) and from 0.6% to 2.9% in females (stomach and cervical cancer respectively).
Whilst the absolute differences of 5-year survival, in Difference A, range from 0.2% (lung and oesophageal cancer) to 2.9% (prostate cancer) in males and from 0.1% to 7.5% in females (lung and cervical cancer respectively). The impact on cancer of the cervix is discussed further in section 6.
Overall, these differences are similar to those published in Tables A3 and A4 of the report for national survival estimates (June 2017). This indicates that changes to the underlying data, as a result of including extra years of cancer diagnoses, do not substantially impact the survival estimates but the choice of age-weights does substantially impact the survival estimates.
Sub-national comparison
Although wide differences in 1-year cancer survival exist across the 44 Sustainability and Transformation Partnerships (STPs), Table 3 shows that overall there is little difference in the variation of survival estimates as a result of applying the updated methodology changes.
Overall, the replicated results have a smaller range compared with the published estimates, indicating there is less variation at this lower geographical level.
Table 3: Comparison of the range in 1-year net survival (%) across the 44 Sustainability and Transformation Partnerships in England
| Published estimates 2008 to 2010 | Updated data with ICSS weights 2007 to 2011 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Range | Min | Max | Range | Percentage point difference of the range | |||
| Bladder | Men | 70.0 | 84.8 | 14.8 | 72.6 | 83.7 | 11.1 | -3.7 | |
| Bladder | Women | 57.2 | 75.8 | 18.6 | 47.1 | 73.2 | 26.1 | 7.5 | |
| Bladder | Persons | 68.6 | 81.5 | 12.8 | 68.3 | 80.8 | 12.5 | -0.3 | |
| Breast | Women | 94.5 | 96.8 | 2.4 | 93.5 | 95.9 | 2.4 | 0.0 | |
| Cervix | Women | 69.7 | 92.1 | 22.4 | 74.2 | 92.4 | 18.2 | -4.2 | |
| Colon | Men | 67.3 | 77.2 | 9.8 | 72.0 | 78.9 | 6.9 | -2.9 | |
| Colon | Women | 68.6 | 78.7 | 10.1 | 70.0 | 80.6 | 10.6 | 0.5 | |
| Colon | Persons | 68.4 | 77.0 | 8.6 | 72.1 | 78.9 | 6.8 | -1.8 | |
| Lung | Men | 26.2 | 33.9 | 7.6 | 25.3 | 35.2 | 9.9 | 2.3 | |
| Lung | Women | 27.5 | 40.1 | 12.5 | 31.2 | 42.2 | 11.0 | -1.5 | |
| Lung | Persons | 27.8 | 36.4 | 8.6 | 28.9 | 38.1 | 9.2 | 0.6 | |
| Oesophagus | Men | 33.0 | 56.3 | 23.3 | 35.5 | 56.1 | 20.6 | -2.7 | |
| Oesophagus | Women | 31.7 | 47.4 | 15.7 | 28.5 | 51.2 | 22.7 | 7.0 | |
| Oesophagus | Persons | 33.4 | 48.1 | 14.7 | 35.7 | 49.5 | 13.8 | -0.9 | |
| Prostate | Men | 89.2 | 95.9 | 6.7 | 92.9 | 96.9 | 4.0 | -2.7 | |
| Stomach | Men | 31.5 | 51.5 | 20.0 | 35.5 | 51.6 | 16.1 | -3.9 | |
| Stomach | Women | 30.2 | 56.0 | 25.7 | 29.1 | 53.6 | 24.5 | -1.2 | |
| Stomach | Persons | 31.0 | 53.2 | 22.2 | 33.4 | 50.4 | 17.0 | -5.2 | |
| Source: National Cancer Registration and Analysis Service within Public Health England; Office for National Statistics | |||||||||
Download this table Table 3: Comparison of the range in 1-year net survival (%) across the 44 Sustainability and Transformation Partnerships in England
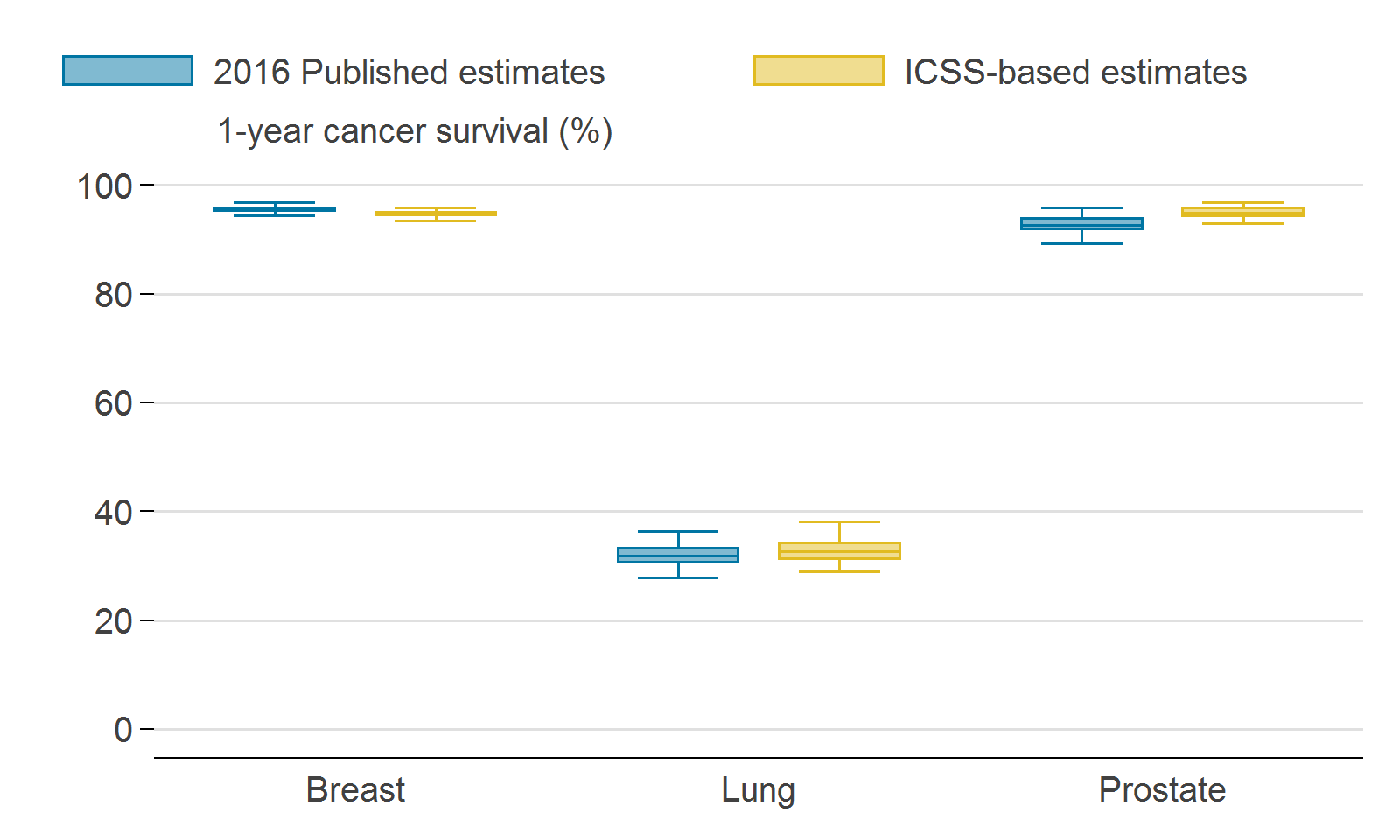
.xls (36.4 kB)Focussing on the three most frequently diagnosed cancers (breast, prostate and lung), the differences between the applied methods for 1-year survival of these three cancer sites are presented in Figure 3, which provides a visual representation of the distribution of 1-year survival cancer estimates. Further information on interpreting a box plot can be found in Appendix 4.
Figure 3: Comparison of the distribution of 1-year survival by Sustainability Transformation Partnerships for breast cancer in women, lung cancer in persons and prostate cancer in men
England, for 2008 to 2010, as published in 2016, and for 2007 to 2011 for the ICSS-based weights
Source: National Cancer Registration and Analysis Service within Public Health England; Office for National Statistics
Download this image Figure 3: Comparison of the distribution of 1-year survival by Sustainability Transformation Partnerships for breast cancer in women, lung cancer in persons and prostate cancer in men
.png (51.2 kB) .xls (25.1 kB)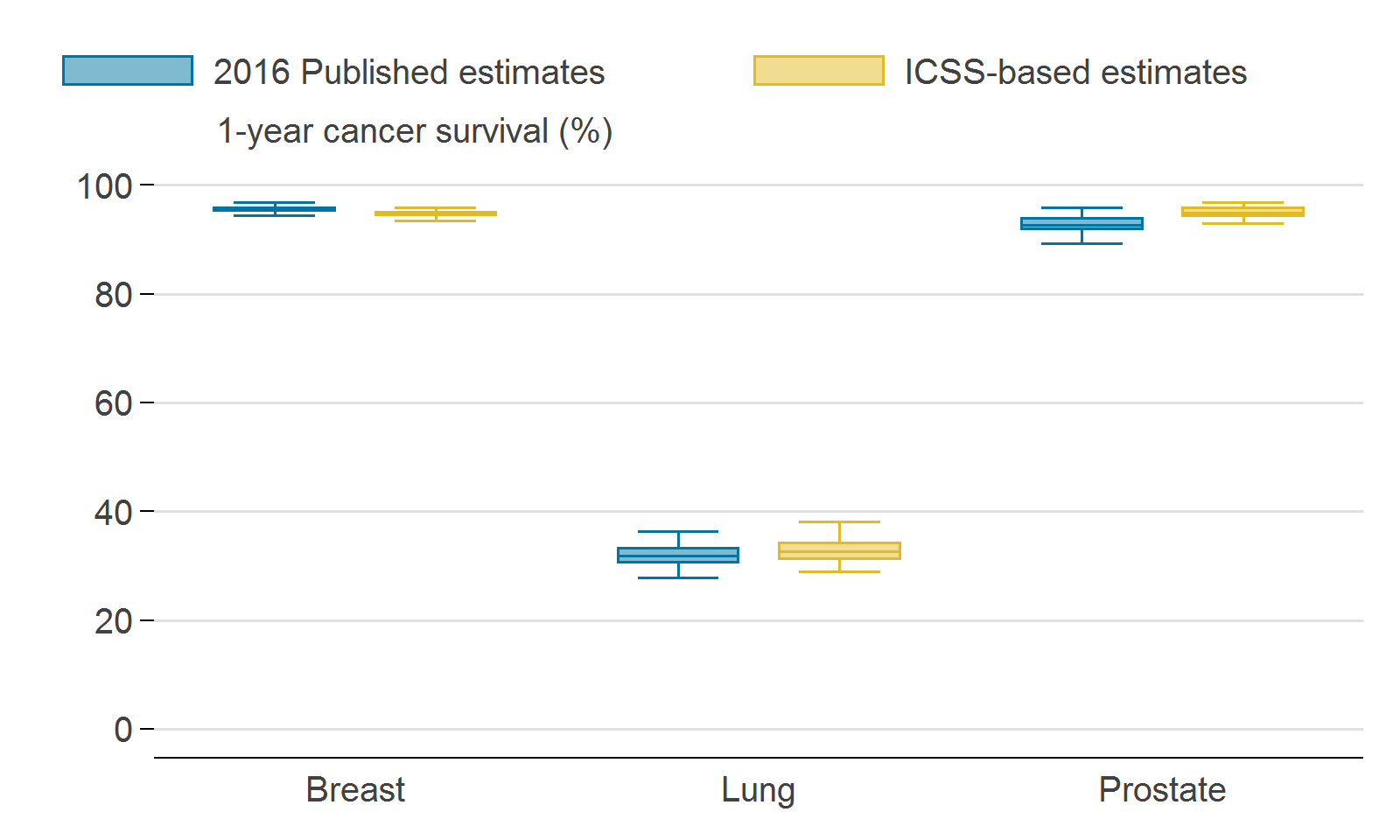{kind=link}
Figure 3 shows that, for breast cancer (in women), the distribution of estimates for 2007 to 2011 was the same as the range of estimates for 2008 to 2010. Table 2 showed that 1-year survival estimates for England decreased by 0.9 percentage points.
The distribution of 1-year survival estimates for prostate cancer (in men) has changed between the two methods as shown in Figure 3. The latest methodology has resulted in a narrower range of 1-year survival estimates for prostate cancer by STPs. Unlike for breast cancer in women (where the new national estimate was lower than the previously published estimates), the latest method has shifted the distribution of 1-year survival estimates to be approximately 2.0 percentage points higher than the previous methodology.
For lung cancer (in persons), the latest methodology has resulted in an increase to the national estimate and to the range of estimates by STP, as shown in Figure 3. The reason for each cancer site being affected differently is because survival estimates are standardised differently depending on the cancer site. Details of the different International Classification of Survival Standard (ICSS) age-standardisation profiles can be found in Table A2.
However, in all three cancers sites, as the distribution of previously published STP estimates and the distribution for the new ICSS-based estimates overlap, we would conclude that the difference between the methodologies is not statistically significant.
Correction 13 April 2018
Table 3, Figure 3 and some text below figure 3 has changed due to a small error in the patient population and updates to the survival estimates used to produce the 2007 to 2011 reference tables. We apologise for any inconvenience.
Back to table of contents6. Why does the change in age-weighting systems result in these differences in the survival estimates?
As a result of adopting the International Classification of Survival Standard (ICSS) weighting, when we consider the combinations of cancer site and sex that form the eight cancers included in this bulletin, for 1-year age-standardised net survival (Table 1, Difference column):
15 cancer sites had an absolute difference of less than 2%
three cancer sites (cervix, prostate, oesophagus) had an absolute difference between 2% and 5%
no cancer sites had an absolute difference greater than 5%
Similarly, for the 5-year age-standardised net survival (Table 1, Difference column):
15 cancer sites had an absolute difference of less than 2%
two cancer sites (breast, prostate) had an absolute difference between 2% and 5%
one cancer site had an absolute difference greater than 5%
The only cancer site that had an absolute difference greater than 5% (in 5-year age-standardised net survival) was cancer of the cervix (females). This is a cancer site with an age profile that is substantially different to the common profile of increasing incidence by age.
The above findings are consistent with the differences reported in Table 2 of the report measuring the impact of updating cancer survival methodologies for national (England) estimates (June 2017). Cancer of the cervix was the only cancer site (reported in both survival bulletins) with an absolute difference greater than 2%. At a national level, the change to ICSS-based age standardisation resulted in a decrease of 3.7 percentage points for 1-year survival and a decrease of 6.8 percentage points for 5-year survival from cervical cancer.
The observed differences may partially be explained by the categorisation of age-groups. The new analysis uses five age groups and weights set out by the ICSS, whereas the previous analyses used six age groups and weights provided in Table A1 (Coleman M 1999). Consequently, the age-group boundaries differ, as does the relative amount of weighting given to younger and older patients.
Back to table of contents7. Overall conclusion of impact
The changes to using five diagnosis years and International Classification of Survival Standard (ICSS)-based weights results in relatively small changes to the 1-year and 5-year survival estimates at the national level. The observed differences are dependent on the cancer type with some sites being greater affected by the move to the ICSS weights.
At Sustainability and Transformation Partnership (STP) level, there are some larger changes, due to the small number of cases diagnosed each year in each age, sex, cancer type and sub-national geography. However, all differences were smaller than 6% for individual cancer types and are consistent with those reported at the national level.
Overall, the changes represent an improvement in both the consistency with the national survival statistical bulletin and the comparability with international survival estimates.
Back to table of contents8. Which publications will be impacted?
To date, Office for National Statistics has published a suite of national and sub-national cancer survival publications.
The method changes outlined in this article will only impact the Geographic patterns of cancer survival in England publication.
The adoption of the International Classification of Survival Standard (ICSS) international cancer patient population for age standardising survival ratios has also been applied to other cancer survival estimates published in partnership with Public Health England, which includes:
- Cancer survival in England: adults
- Cancer survival by stage at diagnosis for England
- Childhood cancer survival
- Index of cancer survival for Clinical Commissioning Groups in England
9. References
Coleman MP, Babb P, Damiecki P, Grosclaude PC, Honjo S, Jones J, Knerer G, Pitard A, Quinn MJ, Sloggett A, De Stavola BL (1999), ‘Cancer survival trends in England and Wales 1971 to 1995: deprivation and NHS region’, Studies on Medical and Population Subjects, Number 61, London: The Stationery Office
Corazziari I, Quinn M, Capocaccia R (2004), ‘Standard cancer patient population for age standardising survival ratios’, European Journal of Cancer, Volume 40, Issue 15, pages 2,301 to 2,316
Li R and others (2014), ‘Control of data quality for population-based cancer survival analysis’ Cancer Epidemiology, Volume 38, pages 314 to 320
Martos C and others (2014) ‘A proposal on cancer data quality checks: one common procedure for European cancer registraies’, European Commission, Joint Research Centre
Pohar PM, Stare J, Estève J (2012), ‘On estimation in relative survival’, Biometrics, Volume 68, pages 113 to 120
World Health Organisation (1994), ‘International statistical classification of diseases and related health problems’, Tenth revision, Geneva: WHO
10. Appendix 1: Weighting
Table A1: Weights for age-standardisation, numbers (%) of adults included in analyses, England and Wales, patients diagnosed 1986 to 1990 (Coleman M 1999)
| Age-group (years) | ||||||||||||||
| 15 - 39 | 40 - 49 | 50 - 59 | 60 - 69 | 70 - 79 | 80 - 99 | All ages | ||||||||
| No. | % | No. | % | No. | % | No. | % | No. | % | No. | % | No. | % | |
| Oesophagus | 167 | 1 | 701 | 3 | 2,442 | 12 | 5,885 | 28 | 7,184 | 35 | 4,351 | 21 | 20,730 | 100 |
| Stomach | 450 | 1 | 1,281 | 3 | 4,293 | 10 | 11,492 | 26 | 15,905 | 36 | 10,164 | 23 | 43,585 | 100 |
| Colon | 894 | 1 | 2,670 | 4 | 7,435 | 11 | 17,461 | 25 | 23,626 | 35 | 16,395 | 24 | 68,481 | 100 |
| Lung | 876 | 1 | 4,585 | 3 | 17,796 | 12 | 51,364 | 35 | 51,775 | 35 | 19,679 | 13 | 146,075 | 100 |
| Breast | 7,092 | 6 | 18,255 | 16 | 23,667 | 20 | 29,809 | 25 | 24,459 | 21 | 14,457 | 12 | 117,739 | 100 |
| Cervix | 5,370 | 28 | 3,650 | 19 | 2,866 | 15 | 3,671 | 19 | 2,473 | 13 | 1,078 | 6 | 19,108 | 100 |
| Prostate | 33 | 0 | 171 | 0 | 2,214 | 4 | 12,598 | 24 | 23,384 | 45 | 13,510 | 26 | 51,910 | 100 |
| Bladder | 650 | 1 | 1,653 | 3 | 5,756 | 12 | 14,269 | 29 | 17,460 | 35 | 9,530 | 19 | 49,318 | 100 |
| All cancers analysed | 15,532 | 3 | 32,966 | 6 | 66,469 | 13 | 146,549 | 28 | 166,266 | 32 | 89,164 | 17 | 516,946 | 100 |
| Source: Coleman M, et al. 1999. Cancer Survival Trends in England and Wales 1971 to 1995 Deprivation and NHS Region. | ||||||||||||||
Download this table Table A1: Weights for age-standardisation, numbers (%) of adults included in analyses, England and Wales, patients diagnosed 1986 to 1990 (Coleman M 1999)
.xls (29.2 kB)
Table A2: International cancer patient population for age-standardising survival ratios (Corazziari I 2004)
| Age Standard for Survival | Population Weights | ||||||
| ICSS 1 | ICSS 2 | ICSS 3 | |||||
| 15 – 44 years | 0.07 | 0.28 | 0.6 | ||||
| 45 – 54 years | 0.12 | 0.17 | 0.1 | ||||
| 55 – 64 years | 0.23 | 0.21 | 0.1 | ||||
| 65 – 74 years | 0.29 | 0.2 | 0.1 | ||||
| 75 – 99 years | 0.29 | 0.14 | 0.1 | ||||
| Age Standard for Survival | Population Weights | ||||||
| ICSS 4 | |||||||
| 15 – 54 years | 0.19 | ||||||
| 55 – 64 years | 0.23 | ||||||
| 65 – 74 years | 0.29 | ||||||
| 75 – 84 years | 0.23 | ||||||
| 85 – 99 years | 0.06 | ||||||
| Groups | Sites | ||||||
| ICSS 1 | All sites except for those listed in the below groups: | ||||||
| ICSS 2 | Nasopharynx, Soft Tissue, Melanoma, Cervix, Brain, Thyroid and Bone | ||||||
| ICSS 3 | Testis, Hodgkin, Acute lymphoblastic leukaemia | ||||||
| ICSS 4 | Prostate | ||||||
| Source: Corazziari I, et al. 2004. “Standard cancer patient population for age standardising survival ratios.” European Journal of Cancer 15: 2307-2316. | |||||||
Download this table Table A2: International cancer patient population for age-standardising survival ratios (Corazziari I 2004)
.xls (29.7 kB)11. Appendix 2: Adult survival comparisons
Table A3: Comparison of 1-year, age-standardised, net survival estimates, patients diagnosed 2007 to 2011 and followed up to 2016, England, for eight cancers
| Cancer | Sex | Published number of patients | Published estimate based on historic weights (2008-2010) | Updated number of patients | New estimates based on ICSS weights (2007-2011) | % point difference | ||
| Bladder | M | 18,859 | 77.8% (77.2 - 78.5) | 31,321 | 78.5% (78.0 - 79.0) | 0.7 | ||
| F | 7,129 | 67.5% (66.3 - 68.7) | 11,867 | 66.7% (65.6 - 67.7) | -0.8 | |||
| P | 25,988 | 75.1% (74.5 - 75.6) | 43,188 | 75.2% (74.7 - 75.7) | 0.1 | |||
| Breast | F | 114,262 | 95.6% (95.5 - 95.8) | 187,710 | 94.7% (94.5 - 94.8) | -0.9 | ||
| Cervix | F | 7,461 | 82.5% (81.6 - 83.5) | 12,273 | 79.6% (78.7 - 80.6) | -2.8 | ||
| Colon | M | 32,688 | 73.5% (73.0 - 74.0) | 53,623 | 75.3% (74.9 - 75.7) | 1.8 | ||
| F | 29,622 | 73.1% (72.6 - 73.6) | 48,997 | 74.5% (74.1 - 74.9) | 1.4 | |||
| P | 62,310 | 73.2% (72.9 - 73.6) | 102,620 | 74.9% (74.6 - 75.2) | 1.7 | |||
| Lung | M | 55,105 | 29.9% (29.5 - 30.3) | 91,854 | 30.7% (30.4 - 31.1) | 0.8 | ||
| F | 43,514 | 34.4% (33.9 - 34.9) | 72,492 | 35.2% (34.8 - 35.5) | 0.8 | |||
| P | 98,619 | 31.9% (31.6 - 32.2) | 164,346 | 32.7% (32.5 - 33.0) | 0.8 | |||
| Oesophagus | M | 13,633 | 41.2% (40.4 - 42.1) | 22,451 | 42.7% (42.0 - 43.4) | 1.5 | ||
| F | 6,668 | 39.6% (38.4 - 40.8) | 11,048 | 42.4% (41.4 - 43.5) | 2.8 | |||
| P | 20,301 | 40.4% (39.7 - 41.0) | 33,499 | 42.3% (41.7 - 42.8) | 1.9 | |||
| Prostate | M | 103,262 | 93.1% (92.8 - 93.3) | 170,340 | 95.1% (95.0 - 95.3) | 2.0 | ||
| Stomach | M | 11,755 | 43.5% (42.6 - 44.5) | 19,529 | 44.9% (44.2 - 45.7) | 1.4 | ||
| F | 6,300 | 42.8% (41.5 - 44.1) | 10,427 | 43.4% (42.4 - 44.5) | 0.6 | |||
| P | 18,055 | 43.2% (42.5 - 44.0) | 29,956 | 44.3% (43.7 - 44.9) | 1.1 | |||
| Source: National Cancer Registration and Analysis Service within Public Health England; Office for National Statistics | ||||||||
Download this table Table A3: Comparison of 1-year, age-standardised, net survival estimates, patients diagnosed 2007 to 2011 and followed up to 2016, England, for eight cancers
.xls (30.2 kB)
Table A4: Comparison of 5-year, age-standardised, net survival estimates, patients diagnosed 2007 to 2011 and followed up to 2016, England, for eight common cancers
| Cancer | Sex | Published number of patients | Published estimate based on historic weights (2008-2010) | Updated number of patients | New estimates based on ICSS weights (2007-2011) | % point difference |
| Bladder | M | 18,859 | 58.0% (57.1 - 58.9) | 31,321 | 57.5% (56.8 - 58.3) | -0.5 |
| F | 7,129 | 47.7% (46.3 - 49.2) | 11,867 | 47.1% (46.0 - 48.3) | -0.6 | |
| P | 25,988 | 55.4% (54.6 - 56.1) | 43,188 | 54.6% (54.0 - 55.2) | -0.8 | |
| Breast | F | 114,262 | 84.9% (84.6 - 85.2) | 187,710 | 82.1% (81.8 - 82.4) | -2.8 |
| Cervix | F | 7,461 | 65.5% (64.3 - 66.7) | 12,273 | 58.0% (56.7 - 59.4) | -7.5 |
| Colon | M | 32,688 | 56.0% (55.3 - 56.7) | 53,623 | 56.6% (56.0 - 57.1) | 0.6 |
| F | 29,622 | 56.2% (55.6 - 56.9) | 48,997 | 56.6% (56.1 - 57.2) | 0.4 | |
| P | 62,310 | 56.0% (55.6 - 56.5) | 102,620 | 56.6% (56.2 - 57.0) | 0.6 | |
| Lung | M | 55,105 | 9.0% (8.7 - 9.2) | 91,854 | 9.2% (9.0 - 9.4) | 0.2 |
| F | 43,514 | 11.9% (11.5 - 12.2) | 72,492 | 12.0% (11.8 - 12.3) | 0.1 | |
| P | 98,619 | 10.3% (10.0 - 10.5) | 164,346 | 10.5% (10.3 - 10.6) | 0.2 | |
| Oesophagus | M | 13,633 | 12.8% (12.1 - 13.4) | 22,451 | 12.6% (12.0 - 13.1) | -0.2 |
| F | 6,668 | 14.9% (14.0 - 15.9) | 11,048 | 14.6% (13.8 - 15.4) | -0.3 | |
| P | 20,301 | 13.2% (12.7 - 13.7) | 33,499 | 13.0% (12.6 - 13.4) | -0.2 | |
| Prostate | M | 103,262 | 81.4% (80.9 - 81.8) | 170,340 | 84.3% (84.0 - 84.6) | 2.9 |
| Stomach | M | 11,755 | 17.7% (16.9 - 18.5) | 19,529 | 18.1% (17.4 - 18.7) | 0.4 |
| F | 6,300 | 19.2% (18.1 - 20.3) | 10,427 | 19.9% (19.0 - 20.8) | 0.7 | |
| P | 18,055 | 18.2% (17.5 - 18.8) | 29,956 | 18.6% (18.1 - 19.1) | 0.4 | |
| Source: National Cancer Registration and Analysis Service within Public Health England; Office for National Statistics | ||||||
Download this table Table A4: Comparison of 5-year, age-standardised, net survival estimates, patients diagnosed 2007 to 2011 and followed up to 2016, England, for eight common cancers
.xls (29.2 kB)12. Appendix 3: Definition of cancers
Table A5: Codes in the International Classification of Diseases, 10th revision (ICD-10)
| Cancer | ICD-10 code |
| Bladder | C67 |
| Breast | C50 |
| Cervix | C53 |
| Colon | C18 |
| Colorectum | C18 to C20 and C21.8 |
| Kidney | C64 to C66 and C68 |
| Lung | C33 and C34 |
| Myeloma | C90 |
| Non-Hodgkin lymphoma | C82 to C85 |
| Oesophagus | C15 |
| Prostate | C61 |
| Rectum | C19 to C20 and C21.8 |
| Stomach | C16 |
| Uterus | C54 to C55 |
| Source: World Health Organization. International Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) and International Classification of Diseases for Oncology, Second Edition (ICD-O). Geneva: World Health Organization. | |
Download this table Table A5: Codes in the International Classification of Diseases, 10th revision (ICD-10)
.xls (27.1 kB)13. Appendix 4: Interpretation of a box plot
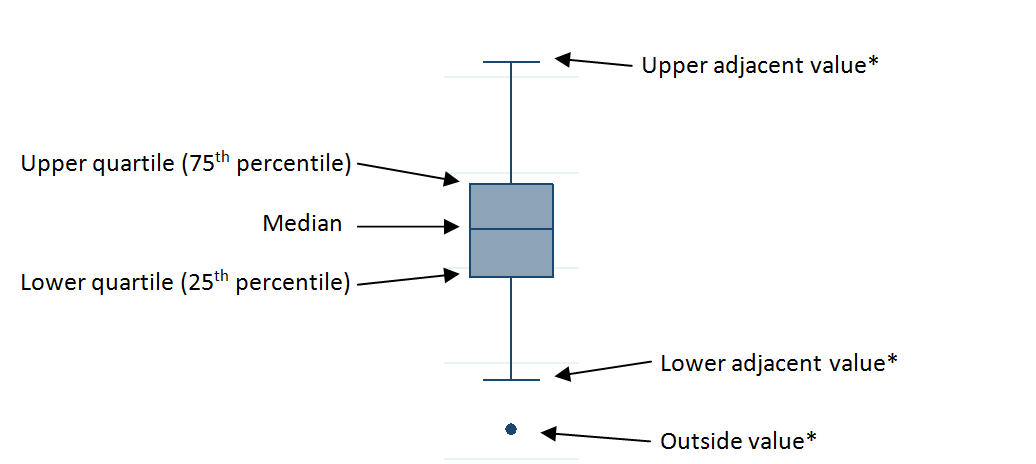
Figure A1: Example of a box plot
Download this image Figure A1: Example of a box plot
.png (13.0 kB)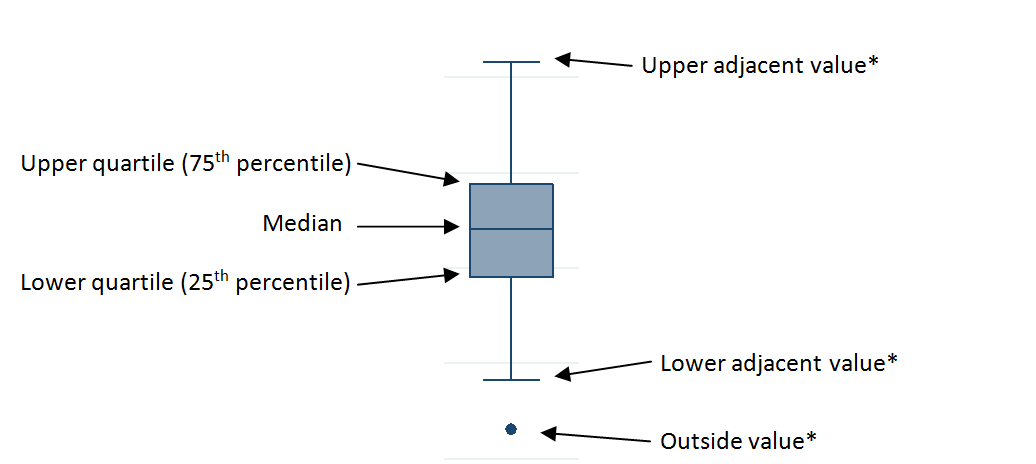{kind=link}
If interquartile range (IQR) equals upper quartile subtract lower quartile, then upper adjacent value, lower adjacent value and outside values are defined as follows:
upper adjacent value: the maximum observed value that is less than upper quartile plus 3 multiplied by IQR
lower adjacent value: the minimum observed value that is greater than lower quartile subtract 3 multiplied by IQR
outside values: any observed value either greater than upper quartile plus 3 multiplied by IQR, or less than lower quartile subtract 3 multiplied by IQR